CT Venography of lower limbs (indirect method)
Last updated June 27, 2026
By Radiohelp Staff

Similar expressions
CTV lower limbs/ CTV lower extremities/ CT venogram/ CT venography/ CECT Venography LL/ CTV LL
Introduction
CT venogram of lower limbs is mainly used to assess pathologies related to lower limb venous system including deep vein thrombosis (DVT), varicose veins, compressing tumors and venous malformations (Klippel-Trenaunay-weber syndrome). There are two techniques in CTV known as direct and indirect, but here we mention about the indirect.
Patient preparation
- Assess suitability to expose radiation and administer intravenous (IV) iodinated contrast media.
- Remove metallic objects in the interested region.
- Remove vein compressing garments such as underwear, stockings, bandages and socks.
- Practice “breath in and hold” breathing technique.
- Place an 18-gauge cannula in a stable vein of a hand.
Patient positioning
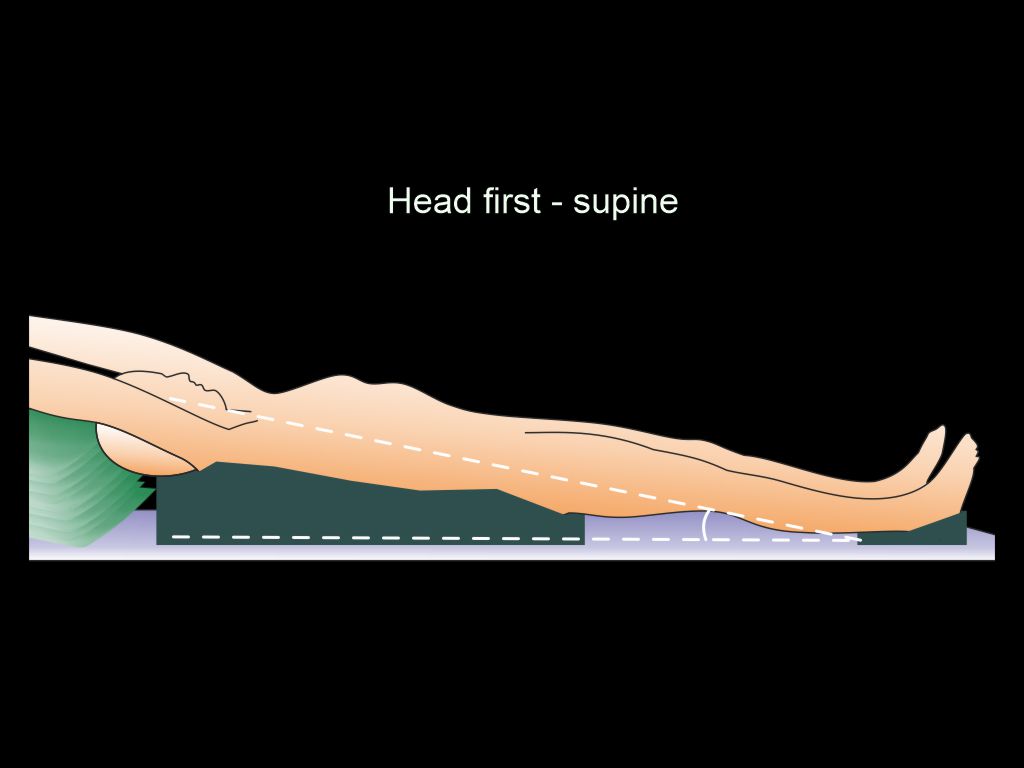
- Position in feet-first supine.
- Place both legs flat on the table.
- Keep padding under buttocks and heels.
Explanation: reduces posterior superficial vein compression due to weight on them.
- Slightly elevate pelvis and upper body compared to heels.
Explanation: delays venous drainage, allowing more time for imaging.
- Keep the interested region in the iso-center of the scanner.
Explanation: this reduces radiation dose to patient and improves image quality.
- Raise hands and keep them beside head.
Explanation: avoids streak artifacts to chest and abdominal area. It also reduces radiation exposure to patient.
Important: this scan is one of the lengthiest body-coverage CT scans. so, move the couch to check the moving range, and avoid tube tangling or accidental stop due to limited couch range.
Scan planning
Venous phase or venogram is acquired either by 2 minutes delayed scan or bolus tracking method.
- Plan the scan slab to cover from diaphragm to ends of lower limbs (toes).
- Place scan direction from head to foot.
Explanation: allows distal venous filling.
- Timing bolus or bolus tracking method is used to start the scan.
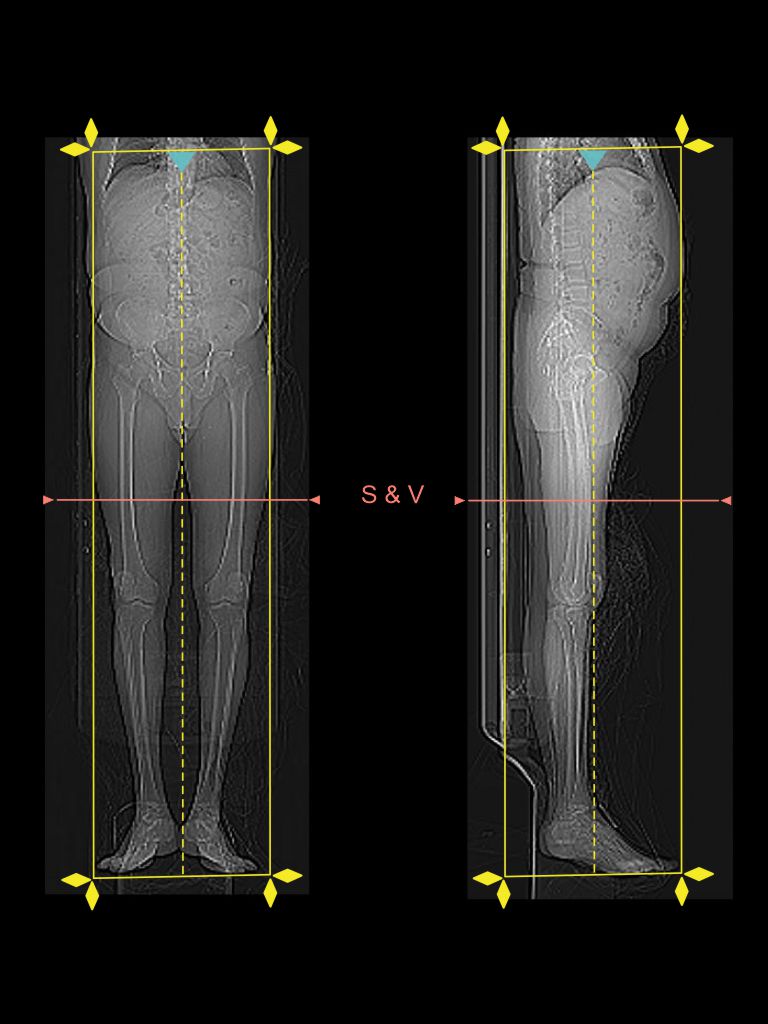
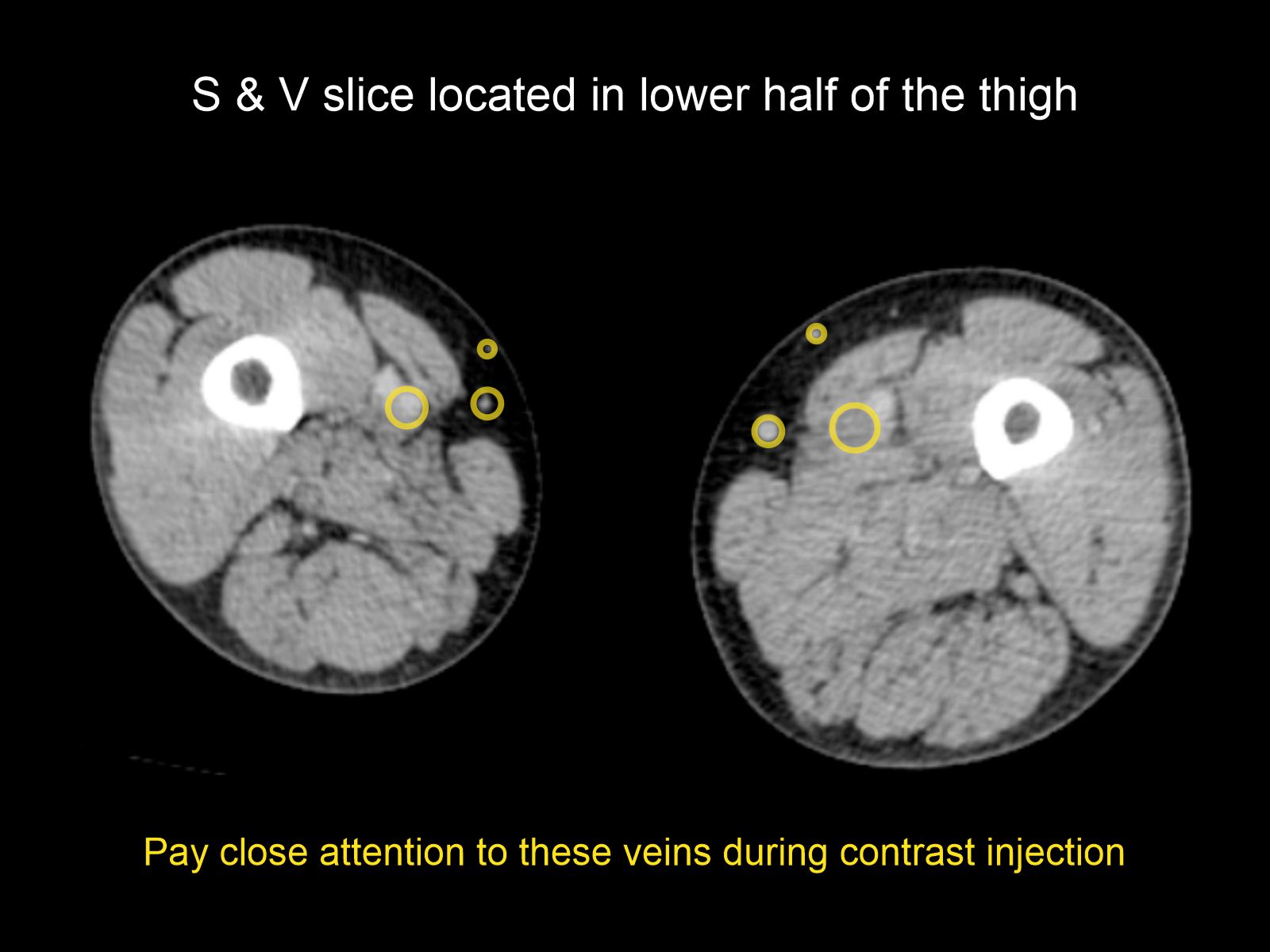
- If bolus tracking method is used, keep scan and view (S & V) slice at the lower half of the thighs.
- Plan 60 seconds delay from contrast injection to S & V initiation.
Explanation: venous flow nearly starts after 70 seconds from contrast injection.
- Use minimum possible kVp according to the body weight of the patient (80kVp for ≤ 75kg and 100kVp for > 75kg).
Explanation: contrast density is reduced in the cycle from arteries to organs and back to veins, therefore use of low kVp can improve the visualization of veins.
- Manually start the venogram when there is adequate superficial venous enhancement - in the S & V scan.
Explanation: automatic triggering can’t be used due to less venous enhancement.
Important: superficial veins are located in the subcutaneous fat tissue. So, attention must be paid for peripheral enhancements in the axial S & V slice. Moreover, lumen diameter of veins are bigger than arteries.
Intra venous (IV) contrast administration.
- Inject 95 ml (body weight of 80kg) of iodinated contrast media at a rate of 4.5 – 5 ml/s with the help of a pressure injector.
- Inject 70 ml of saline flush just after completing the contrast volume.
Explanation: flushes remaining contrast in veins of the injected hand and helps to maintain contrast flow for a longer time.
Post-processing
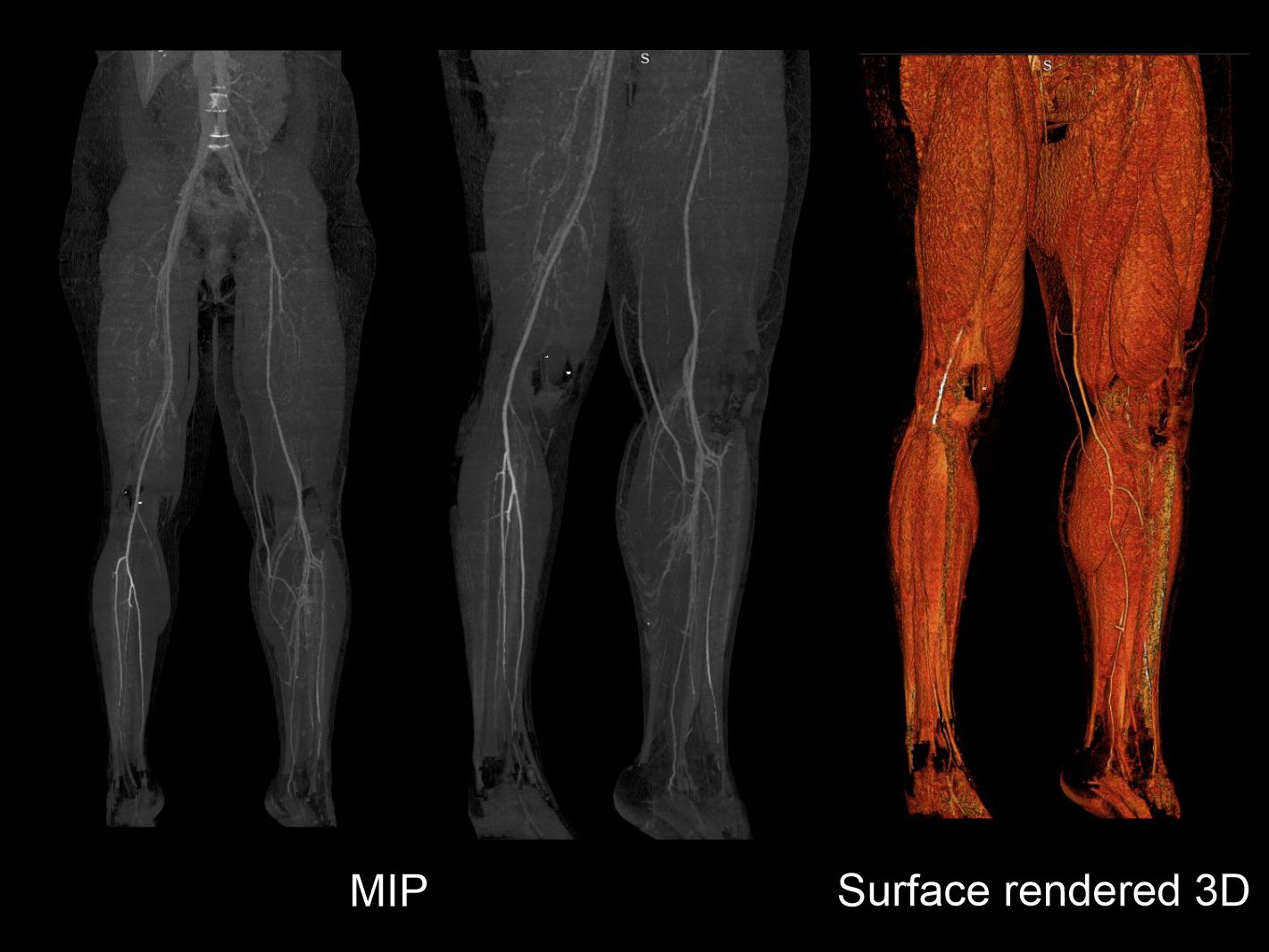
Diagnosis is mostly carried out using MPR, and axial images are prominently used. Enhanced veins of indirect CTV have low density values, therefore rendering MIP (maximum intensity projection) and 3D surface shaded images are challenging. However, those can be rendered to some extent by widening the density window, and using pre and post-contrast phases for subtraction – radiation exposure is higher compared to single acquisition.
- Axial, sagittal and coronal images in both bone (WW: 3500, WL: 350) and soft tissue window (WW: 500, WL: 50) with ≤ 2mm slice thickness.
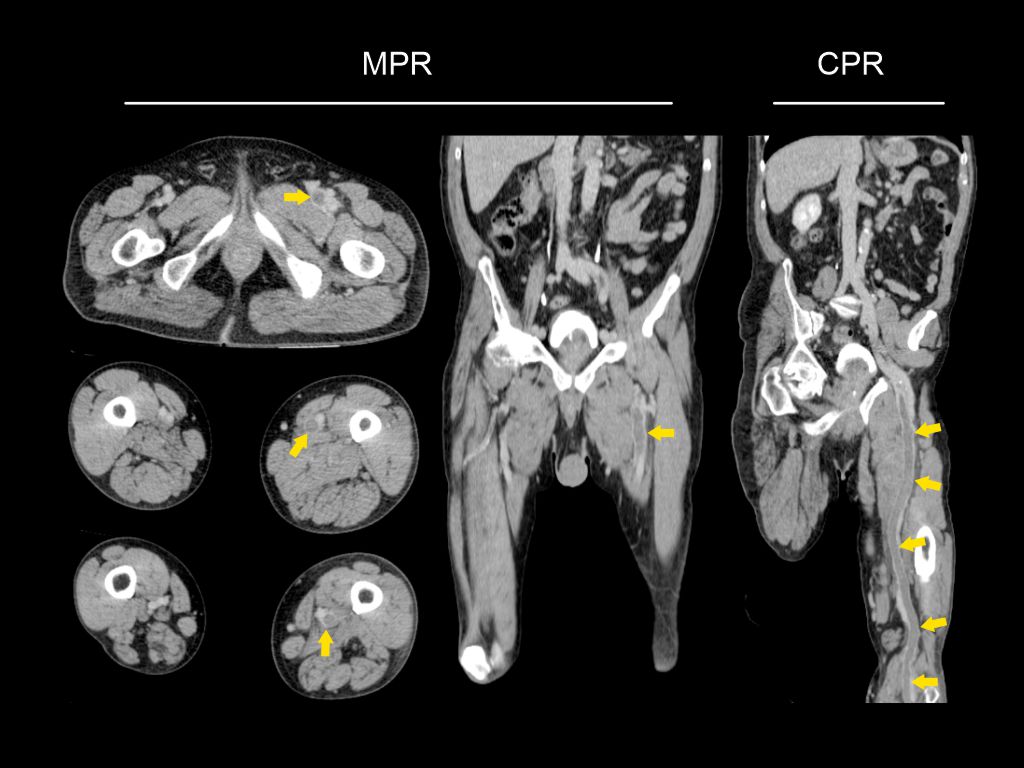
- 3D surface shaded images and MIP images to demonstrate lower limb veins.
Reference
- Ghaye B, Szapiro D, Willems V, Dondelinger RF. Pitfalls in CT venography of lower limbs and abdominal veins. AJR Am J Roentgenol. 2002 Jun;178(6):1465-71. doi: 10.2214/ajr.178.6.1781465. PMID: 12034620.
- Lee W, Chung JW, Yin YH, Jae HJ, Kim SJ, Ha J, Park JH. Three-Dimensional CT venography of varicose veins of the lower extremity: image quality and comparison with doppler sonography. AJR Am J Roentgenol. 2008 Oct;191(4):1186-91. doi: 10.2214/AJR.07.3471. PMID: 18806163.
- Ana Marija Alduk, M. P. (2018, July). CT Venography: Technique and Indications. Retrieved from www.evtoday.com: https://evtoday.com/articles/2018-july/ct-venography-technique-and-indications
- Tran TT, Kristiansen CH, Thomas O, Roy S, Haidl F, Ashraf H, Kløw NE, Stavem K, Lauritzen PM. Indirect CT venography of the lower extremities: impact of scan delay and patient factors on contrast enhancement and examination quality. Eur Radiol. 2022 Nov;32(11):7946-7955. doi: 10.1007/s00330-022-08841-0. Epub 2022 May 12. PMID: 35554646; PMCID: PMC9668790.
- Cho ES, Chung JJ, Kim S, Kim JH, Yu JS, Yoon CS. CT Venography for Deep Vein Thrombosis Using a Low Tube Voltage (100 kVp) Setting Could Increase Venous Enhancement and Reduce the Amount of Administered Iodine. Korean J Radiol. 2013 Mar-Apr;14(2):183-193.
- Sanjit Tewari, MD, Chair, Kevin W. Dickey, MD, FACR, Thomas J. Ward, MD, Christopher D. Yeisley, MD, Mark Baerlocher, MD, & Kush R. Desai, MD. (2023). ACR–SIR Practice parameter for the performance of diagnostic infusion venography. Retrieved from www.gravitas.acr.org