Triple Phase CT Abdomen
Last updated July 01, 2026
By Radiohelp Staff

Similar expressions
CT contrast abdomen/ CT contrast liver/ CT multiphase abdomen/ CT triple-phase liver/ CT triple-phase abdomen/ CT four-phase liver/ CT four-phase abdomen/ CECT abdomen/ CT abdomen contrast/ CECT abdomen and pelvis
Introduction
Triple Phase CT Abdomen is mainly helpful in the detection of conditions within the abdominal cavity, such as neoplasms, trauma, congenital abnormalities, and for surgical planning. Contrast media is used for this scan to recognize and categorize pathologies.
Patient preparation
- Explain the procedure clearly and kindly.
- Check the suitability to administer intra-venous (IV) iodinated contrast.
- Place an Intra venous (IV) cannula in a stable vein for contrast injection – pink-20G cannula.
- Instruct the patient to breath in and hold during the scan.
Explanation: avoids motion unsharpness of liver, pancreas and kidneys.
- Explain the burning sensation during contrast injection.
- Check the ability to expose radiation.
- Ask the patient to remove metals related to the interested region.
- Use gastro-intestinal contrast media if needed.
Explanation: Intraluminal contrast media is mainly used to distend bowel and improve visualization of bowel pathologies. Contrast administration is usually done orally or rectally, or both. Oral administration fills stomach and small bowel. In contrast, rectal administration fills mainly the colon. Mannitol, which has slow absorption rate, can be given orally to fill the entire GI track. In comparison, water is only capable of reaching the proximal part of bowel due to its rapid absorption if administered orally.
There are three major types of GI contrast media known as neutral, positive and negative. They are selected according to patient condition and diagnostic need.
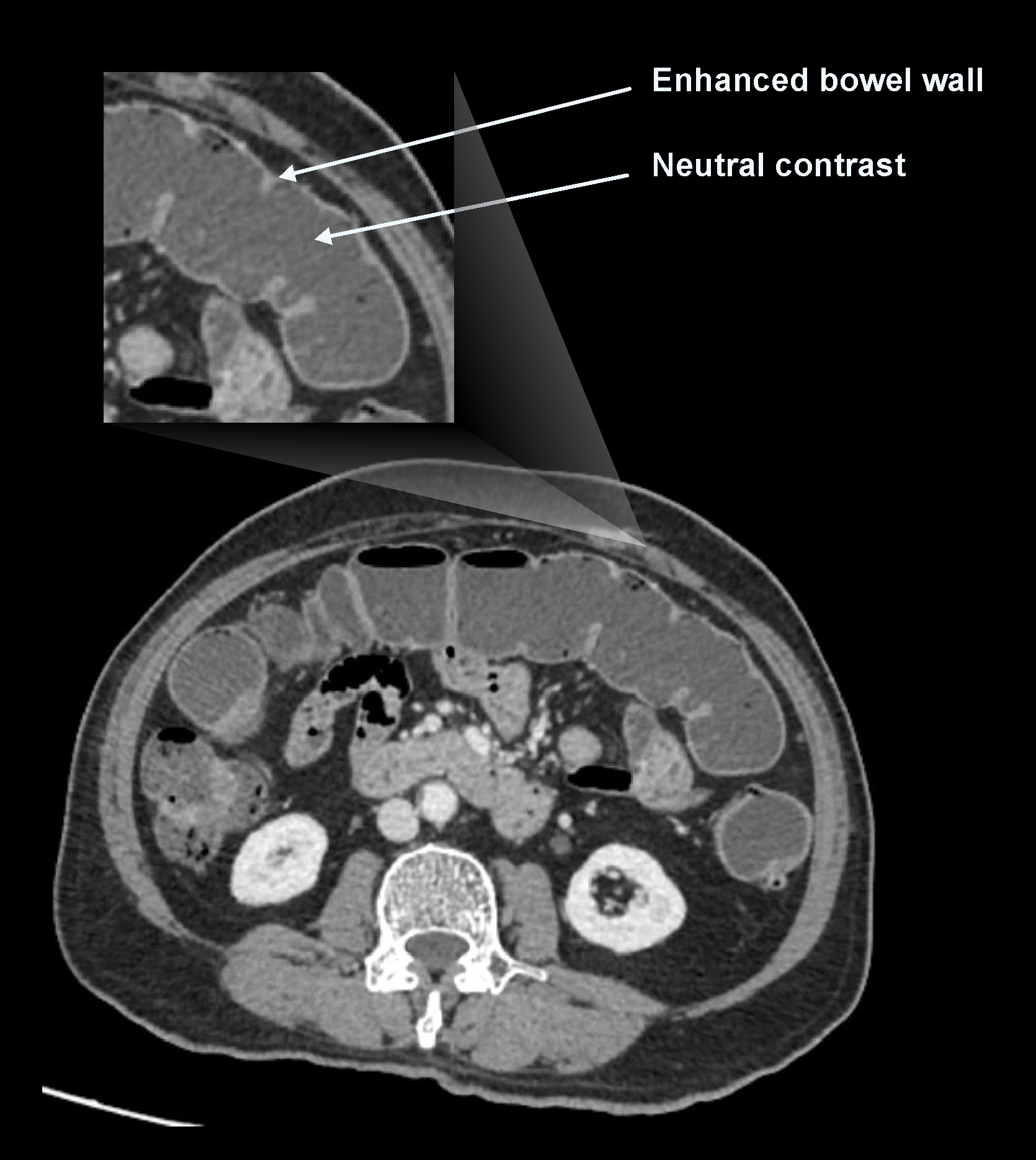
a. Neutral contrast media
Contrast media in this category have a density equal to water (nearly zero Hounsfield unit (HU) value). Water and mannitol can be used as neutral contrast media. Neutral contrast distends bowel, and their neutral appearance compared to bowel wall helps to differentiate bowel enhancement patterns and masses. However, they may obscure the visualization of extraluminal pathologies such as fluid collections, abscesses, masses, fistulas and perforations.
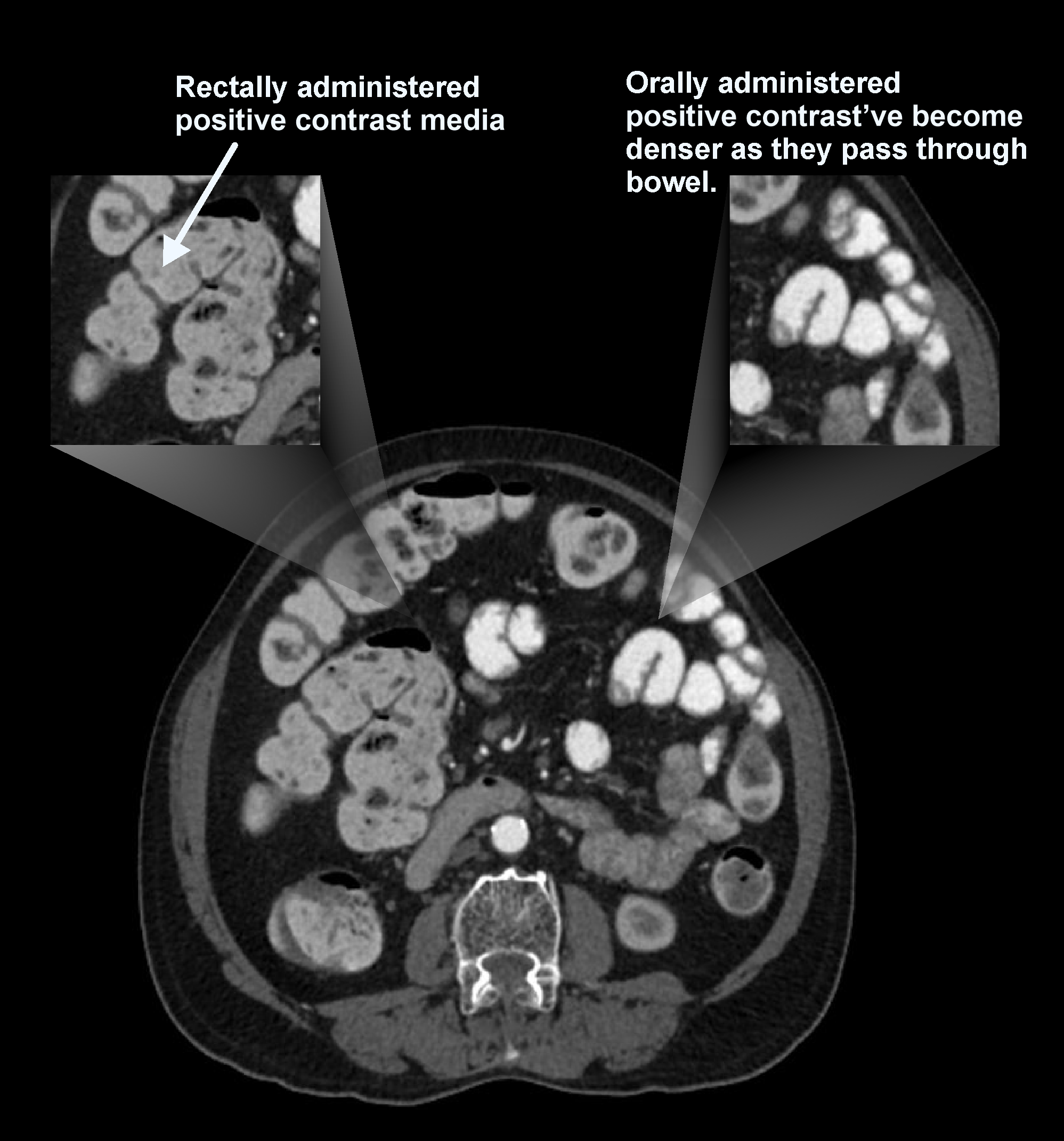
b. Positive contrast media
Contrast media in this category have the highest density (positive HU value), which appear bright on images. Iodinated contrast and barium sulphate are commonly used as positive contrast. Their brighter appearance in bowel lumen help to identify abscess, suspected leaks, peritoneal implants, and intra-abdominal tumors. Nevertheless, positive contrast obscures the visualization of bowel wall enhancement patterns, and can’t be used in angiograms where 3D-reformation is needed.
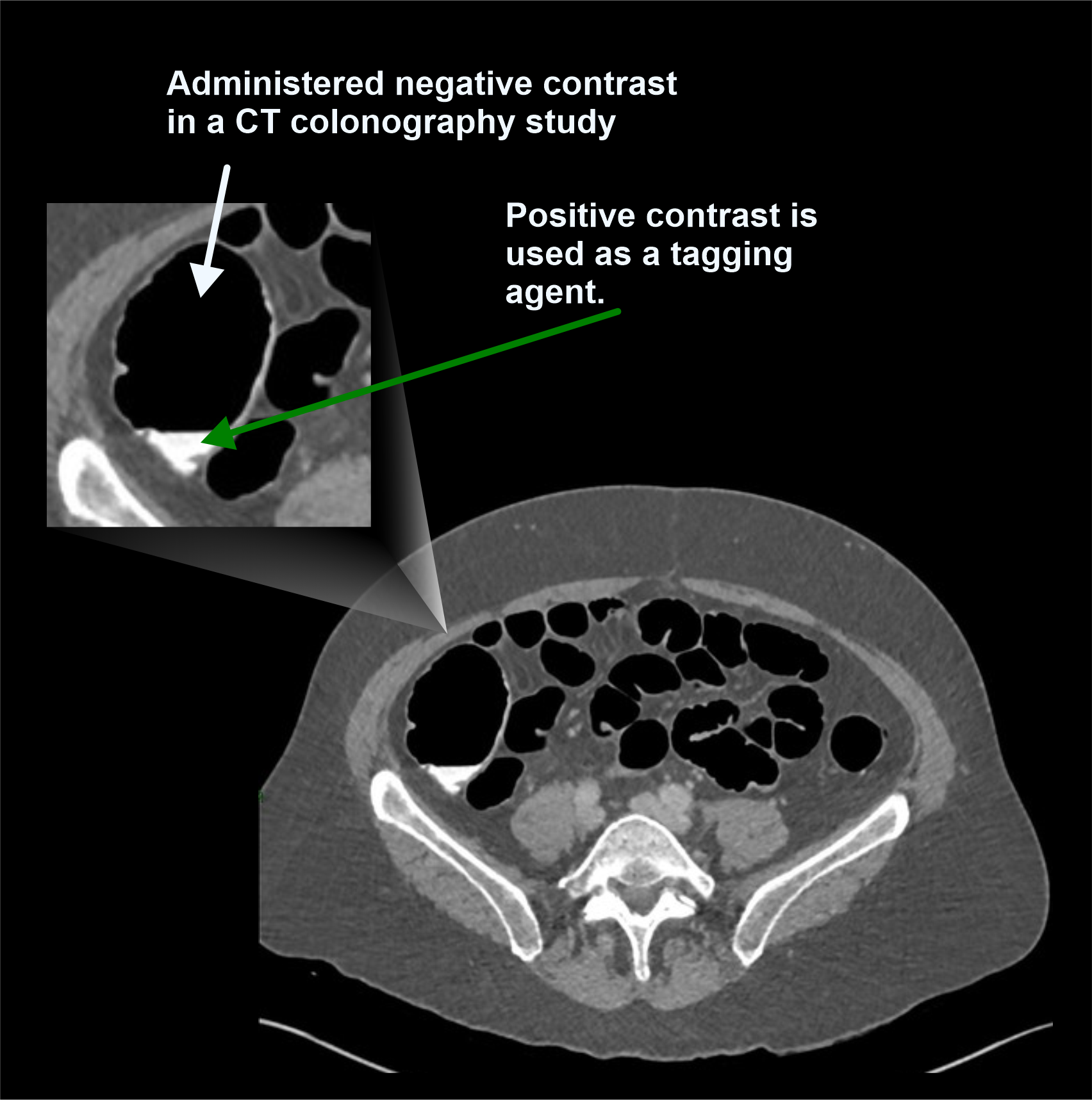
C. Negative contrast media
Contrast media in this category have the lowest density (negative HU value), and appear dark on images. Room air and carbon dioxide (CO2) are commonly used as negative contrast, and they are used to distend bowel in CT colonography scans.
Patient positioning
- Position the patient in feet first and supine.
- Center the scanning area in the scanner iso-center [6].
Explanation: this reduces overall radiation exposure and increases image quality.
- Place both hands above the head.
Explanation: this reduces streak artifacts from the hands, also it avoids unnecessary radiation exposure to the hands.
- Keep the arm with the IV cannula strait.
Explanation: to facilitate contrast flow.
- Plan the scout starting point at the nipple level.
Scan planning
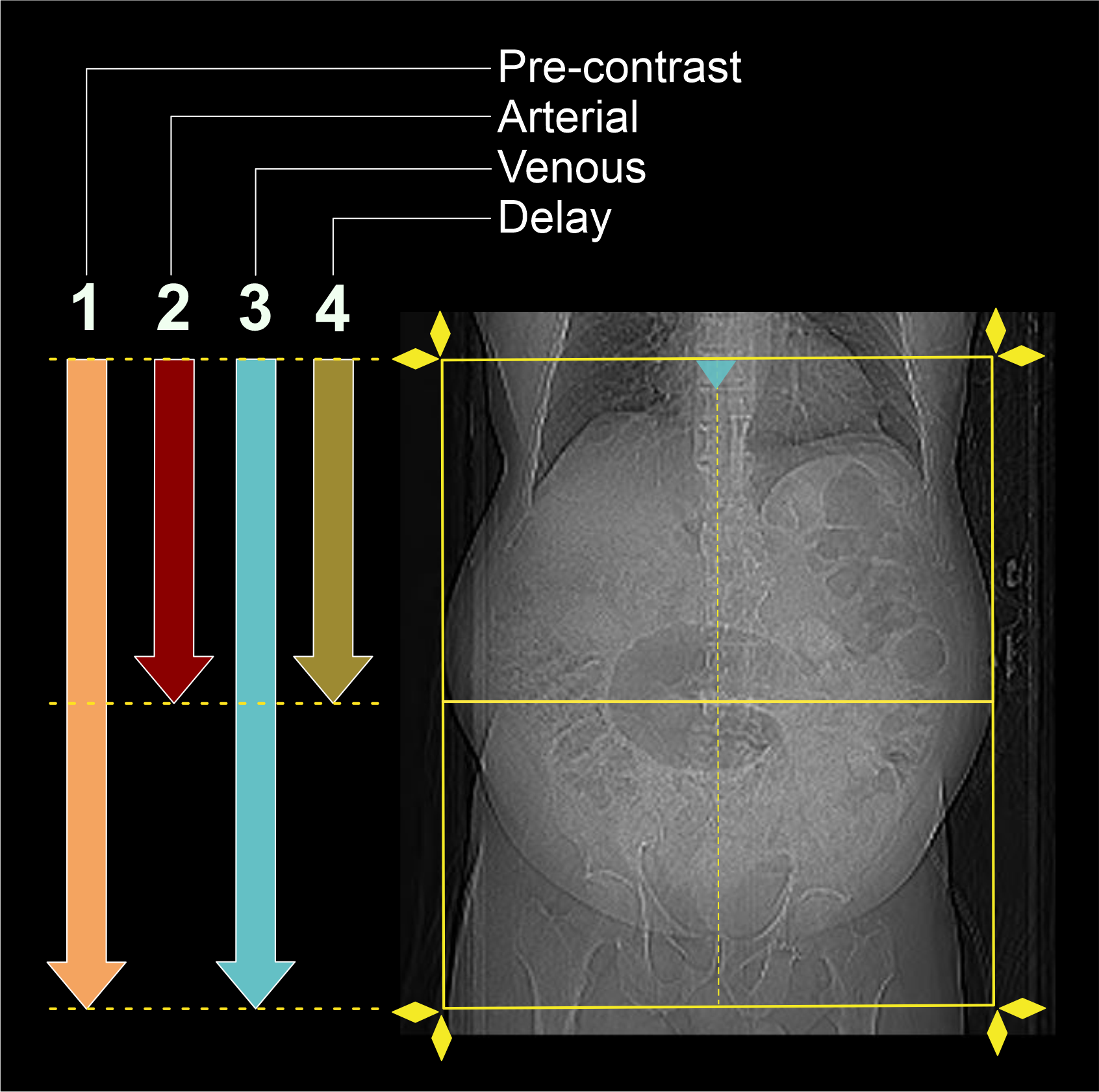
- There are generally 4 phases in this scan.
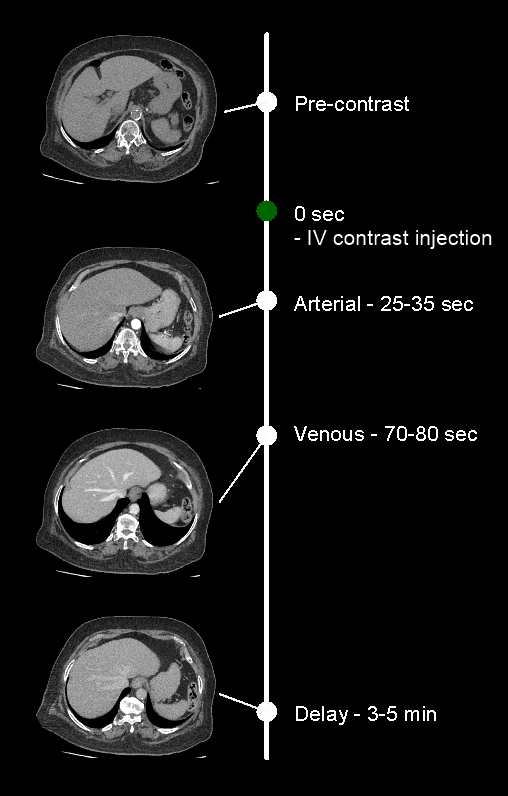
- Plan pre-contrast scan to cover from the dome of the diaphragm to a level just below the ischial tuberosities.
- Plan arterial and delayed phases to cover form the Dome of the diaphragm to the upper margin of the sacroiliac joints.
- Plan portal-venous phase to cover form the Dome of the diaphragm to a level just below the ischial tuberosities.
Important: covering areas may be changed according to the patient condition and theradiologist’s preference.
- Set the phase initiation.
Explanation: either triggering or timing method can be used to initiate phases on time.
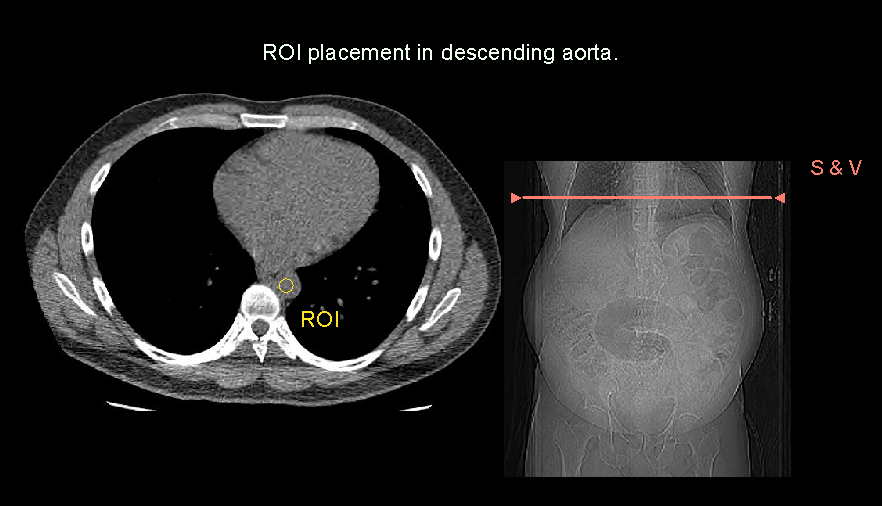
a. Bolus tracking method
Scan-and-view slice (S and V) is placed just above the diaphragm, and threshold value is setto 180, and triggering ROI is placed in the descending aorta. Keep a ten seconds gap between the contrast initiation point and triggering point. Either automatic or manual triggering can be used. Refer thoracic aortogram article for more details.
b. Timing bolus method
Time is set according to the needed phase. They are counted from the contrast initiation point. Triggering time may be placed in seconds, for instance, 30 seconds for arterial phase.
Intravenous (IV) contrast infusion
- Generally, a volume of 75 to 80 ml of iodinated contrast can be injected at a flow rate of 3-3.5ml/s – this is for a patient with a body weight of 75 to 80 kg.
- Inject 50ml of saline flush following the contrast injection.
Explanation: flushes remaining contrast in the veins of the injected hand, and maintainscontrast flow for a longer time.
- Conduct all phases under arrested inspiration.
Post-processing
- Axial, coronal and sagittal images in soft-tissue window (WW:500, WL:50) with ≤ 5mm slicethickness. Refer to NCCT abdomen for images.
- Axial reconstruction in bone window (WW: 3500, WL: 350) with ≤ 3mm slice thickness.
Reference
- Han, J. K., Choi, B. I., Kim, A. Y., & Kim, S. J. (2001). Contrast media in abdominal computed tomography: optimization of delivery methods.Korean journal of radiology, 2(1), 28–36.https://doi.org/10.3348/kjr.2001.2.1.28
- Pickhardt PJ. Positive Oral Contrast Material for Abdominal CT: Current Clinical Indications and Areas of Controversy.AJR Am J Roentgenol. 2020 Jul;215(1):69-78. doi: 10.2214/AJR.19.21989.Epub 2020 Jan 8. PMID: 31913069.
- Kulkarni, N. M., Fung, A., Kambadakone, A. R., & Yeh, B. M. (2021). Computed Tomography Techniques, Protocols, Advancements, and Future Directions in Liver Diseases.Magnetic resonance imaging clinics of North America, 29(3), 305–320. https://doi.org/10.1016/j.mric.2021.05.002
- Brown, M. P. (2024). Abdominal CT: Phases. Retrieved from www.litfl.com.
- Almohammed, H. I., Elshami, W., Hamd, Z. Y., & Abuzaid, M. (2024). Optimizing CT Abdomen-Pelvis Scan Radiation Dose: Examining the Role of Body Metrics (Waist Circumference, Hip Circumference, Abdominal Fat, and Body Mass Index) in Dose Efficiency.Tomography (Ann Arbor, Mich.), 10(5), 643–653. https://doi.org/10.3390/tomography10050049
- Romanyukha, A., Nzitunga, P. S., & Dolcet, A. (2022, April 28). CT patient positioning plays key role in radiation dose reduction.www.auntminnie.com.
- Olga R. Brook, MD, Chair, Jessica Kurian MD, Alec Megibow, MD, MPH, FACR, & Michael Furman,MD. (2021). ACR–SABI–SAR–SPR practice parameter for the performance of computed tomography (CT) of the abdomen and computed tomography (CT) of the pelvis.Retrieved from www.gravitas.acr.org.
- Patel, A., Lalwani, N., & Kielar, A. (2024). Use of oral contrast in 2024: primer for radiologists.Abdominal radiology (New York), 49(8), 2953–2959. https://doi.org/10.1007/s00261-024-04409-2
- Callahan MJ, Talmadge JM, MacDougall R, Buonomo C, Taylor GA. The Use of Enteric Contrast Media for Diagnostic CT, MRI, and Ultrasound in Infants and Children: A Practical Approach.AJR Am J Roentgenol. 2016 May;206(5):973-9. doi: 10.2214/AJR.15.15437. Epub 2016 Feb 25. PMID: 26915020.
- Vasanawala SS, Desser T, Jeffrey RB. Value of delayed imaging in MDCT of the abdomen and pelvis.AJR Am J Roentgenol. 2006 Jul;187(1):154-63. doi: 10.2214/AJR.05.0148. Erratum in: AJR Am J Roentgenol. 2006 Sep;187(3):600. Jeffrey, R Brooke [added]. PMID: 16794170.