CT abdominal aorta
Last updated January 25, 2026
ADVERTISEMENT
Similar expressions
CT abdominal aortogram/ CT abdominal aorta/ CT abdominal angio/ CT aortogram/ CT abdominal aorta/ CECT abdominal aortogram
Introduction
CT abdominal aorta is performed to assess pathologies associated with the abdominal aorta. Either whole aorta or abdominal aorta is acquired, depending on the patient's condition–refer thoracic aortogram article. There are multiple phases in this study that perform pre and post contrast, but some of the phases can be excluded according to the purpose. Non-contrast phase is important as the contrast phase for identifying stents and calcifications, and evaluating mural or extravascular hemorrhages. This study helps to diagnose conditions such as aortic aneurysms, aortic stenosis, aortic rupture, aortic dissection and intra-mural hematoma.
Patient preparation
- Explain the procedure clearly and kindly.
- Check contraindications for contrast media administration and radiation exposure.
- Remove metals related to the interested region.
- Place an Intra venous (IV) cannula in a stable vein of the right arm – green-18G cannula.
Explanation: green cannula has higher lumen diameter, which can withstand higher flow rate.A right arm injection is preferred in thoracic CTA because to avoid streak artifacts from undiluted contrast media in the left brachiocephalic vein.
- Explain and practice breath in and hold technique.
Explanation: avoids motion un-sharpness of organs and blood vessels.
Patient positioning
- Position the patient in supine and feet first on the imaging couch.
- Center the scanning area in the scanner iso-center [6].
Explanation: this reduces overall radiation exposure and increases image quality.
- Raise both hands above the head and place a positioning aide under hands.
Explanation: hands beside the trunk give streak artifacts and increase radiation exposure.
- Keep the arm with the IV cannula strait.
Explanation: to facilitate contrast flow.
- Plan the scan starting point at the lower neck for whole aorta, and at the nipple level forabdominal aorta.
ADVERTISEMENT
Scan planning
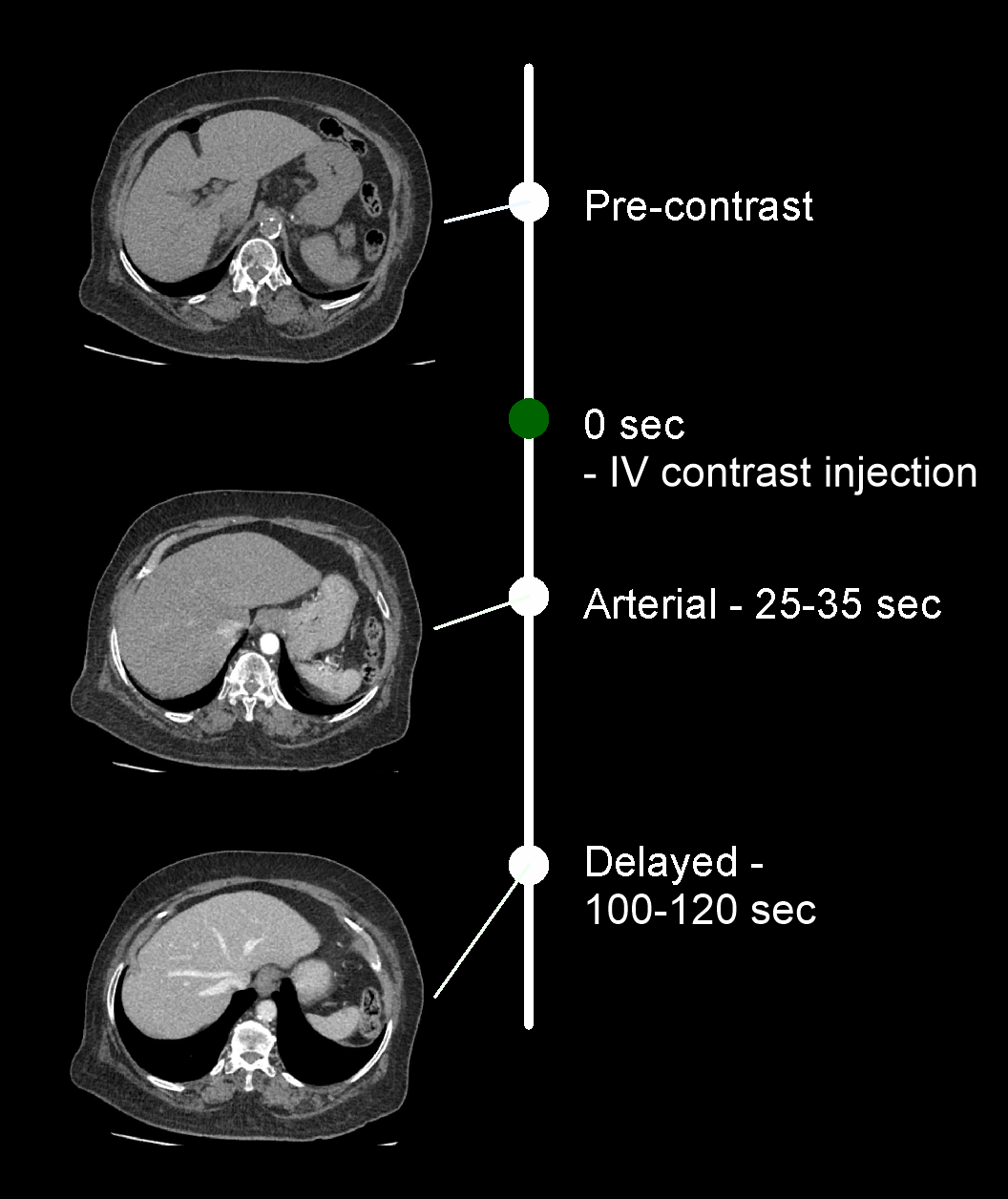
Usually, there are three steps in the scan: pre-contrast, arterial and delayed. First two steps are usually performed in this scan but delayed phase is equally important to detect adequate filling of aneurysms or recognize delayed leakages.
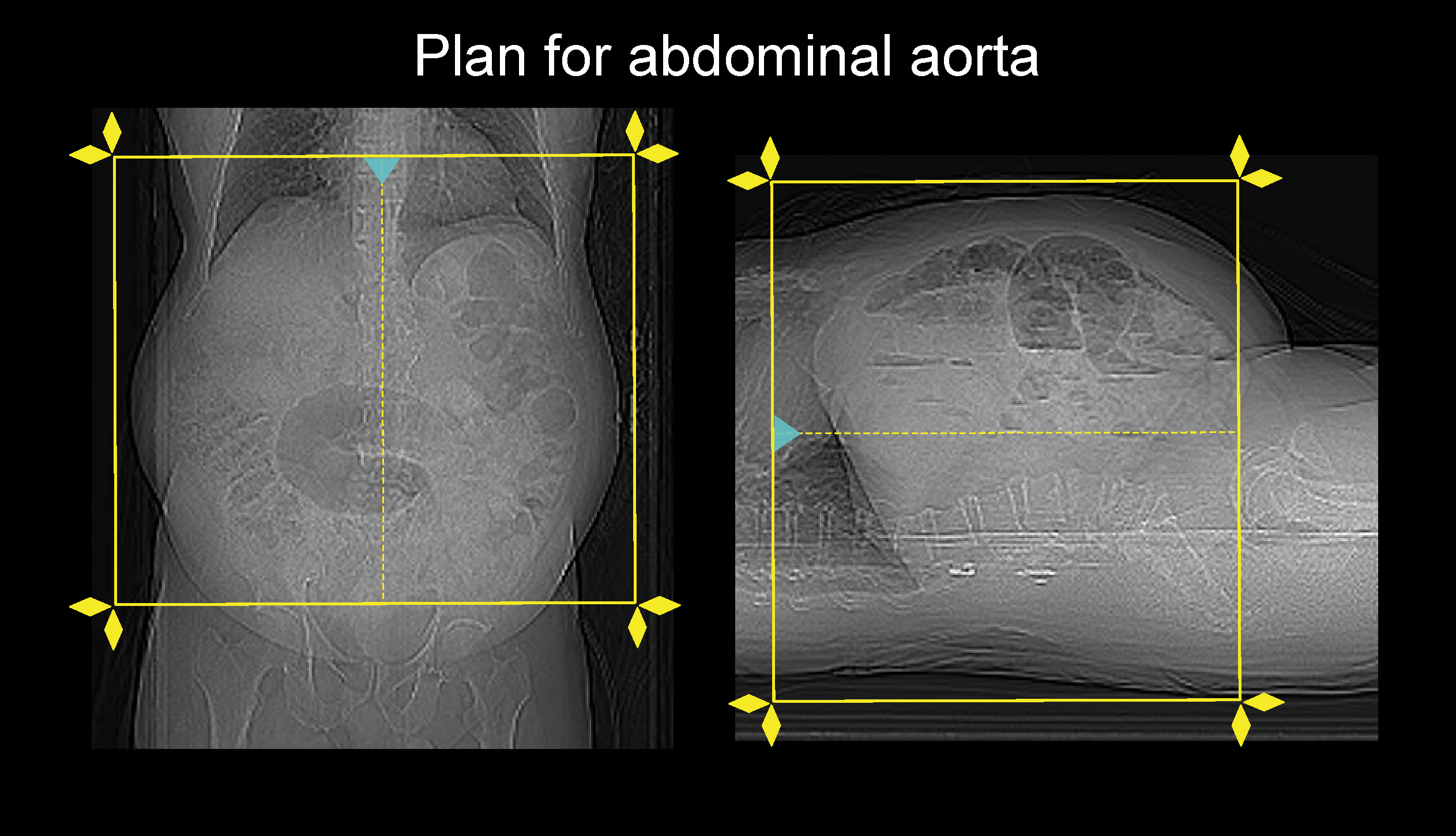
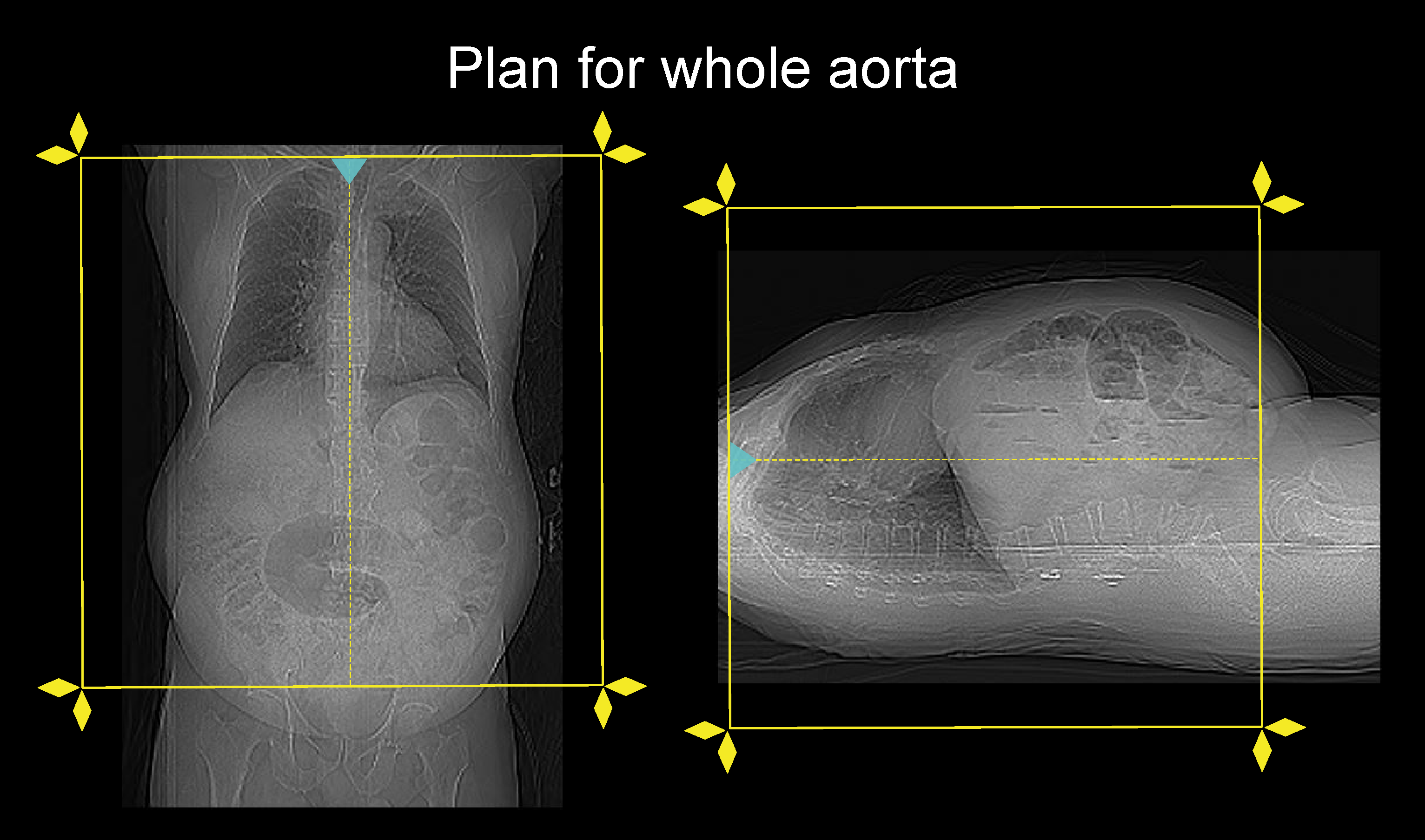
For abdominal aortogram, plan all three steps to cover from dome of the diaphragm to a point just above the hip joints. For whole aortogram, all phases are planed from lung apex to a level just above hip joint, and must use ECG gating to minimize motion artifacts from the heart – refer thoracic aortogram article for details.
- Set the phase initiation.
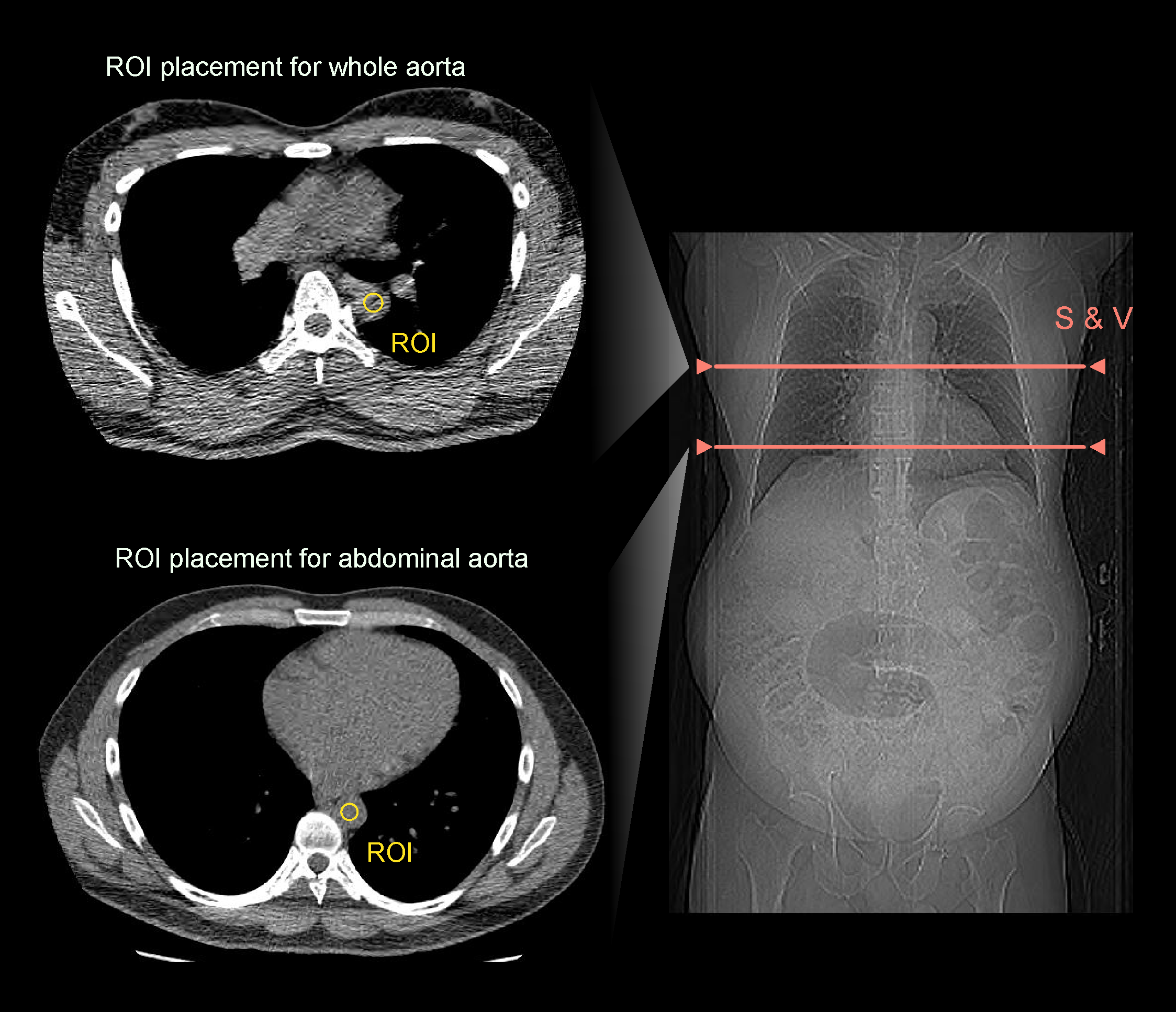
Explanation: triggering method can be used to initiate angiographic phase on time. For abdominal aorta, scan-and-view slice (S and V) is placed just above the diaphragm. Place S and V slice in the mid chest for whole aorta, and threshold value is set to 180, and triggering ROI is placed in the descending aorta. Keep a ten seconds gap between the contrast initiation point and triggering point. Either automatic or manual triggering can be used. Refer thoracic aortogram article to know about triggering techniques.
Intravenous (IV) contrast infusion
- For abdominal aortogram, inject 70 ml (for a patient with 70-80kg body weight) of iodinated contrast media at a rate of 4.5-5ml/s.
- For whole aortogram, inject 80 ml (for a patient with 70-80kg body weight) of iodinated contrast media at a rate of 4.5-5ml/s.
- Inject 50-60ml of saline flush following the contrast injection.
Explanation: flushes remaining contrast in the veins of the injected hand, and maintains contrast flow for a longer time.
- Conduct all phases under arrested inspiration.
Important: when administering IV contrast, factors such as injection rate, contrast volume, and infusion technique might be changed according to the patient body weight, patient condition, scan coverage, departmental protocol and CT scanner model. So, an experienced user is essential here for the safety of the patient.
ADVERTISEMENT
Post-processing
- Multiplanar reconstruction (MPR) images for all phases in soft-tissue window (WW:500, WL:50) with slice thickness ≤ 5mm.
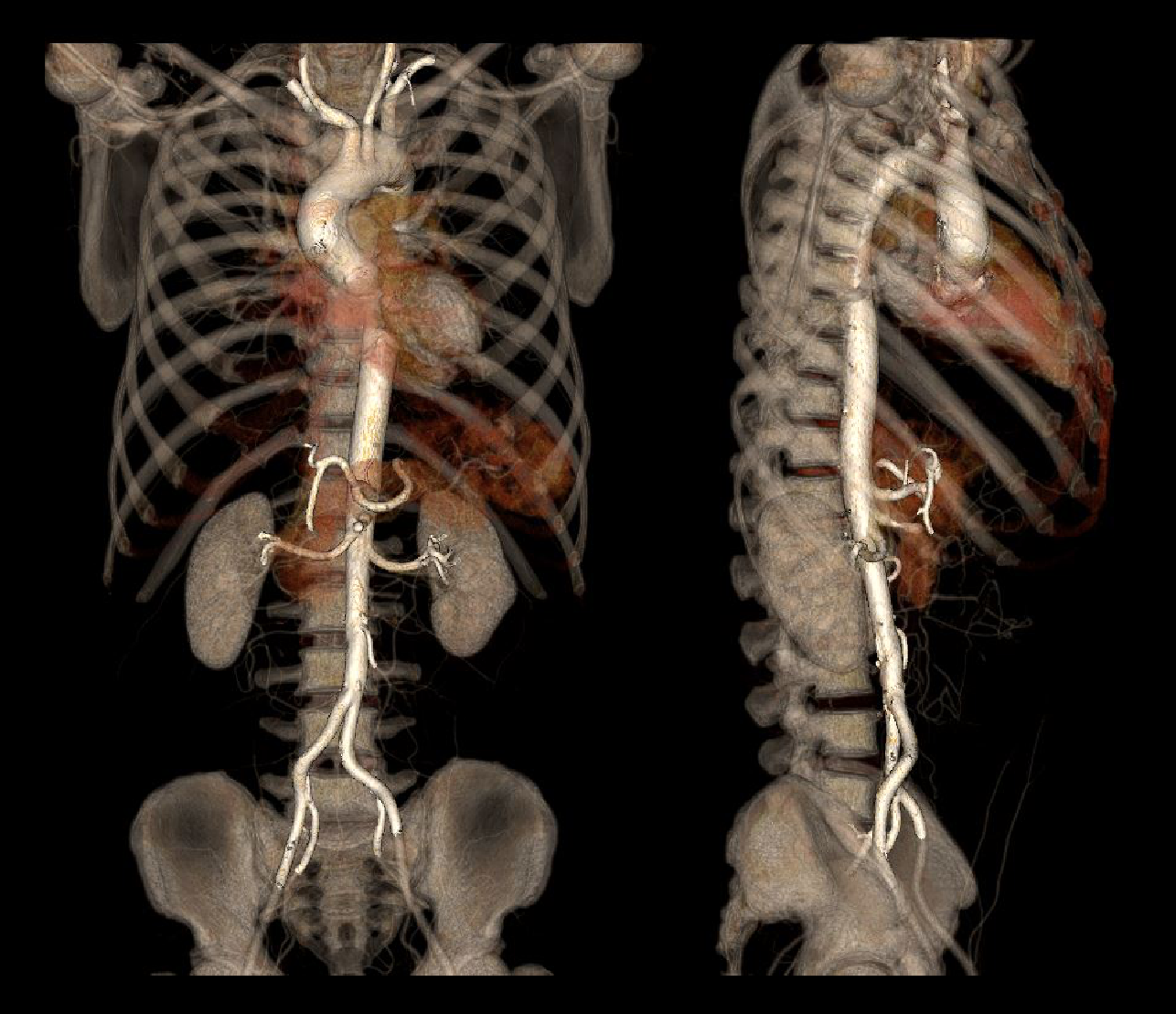
- Surface rendered 3D and Maximum intensity projection (MIP) images of abdominal aorta.

- Curved planar reformation (CPR) images of aorta.
- Axial images in bone window (WW: 3500, WL: 350) with ≤ 3mm slice thickness.
Refer thoracic aortogram article for more images.
Reference
- Steven S. Raman, MD, Chair, Dorothy Gilbertson, MD, & Charles White, MD. (2021). ACR–NASCI–SIR–SPR Practice parameter for the performance and interpretation of body computed tomography angiography (CTA).Retrieved from www.gravitas.acr.org.
- Sparks AR, Johnson PL, Meyer MC. Imaging of abdominal aortic aneurysms. Am Fam Physician. 2002 Apr 15;65(8):1565-70. PMID: 11989632.
- Wu W, Budovec J, Foley WD. Prospective and retrospective ECG gating for thoracic CT angiography: a comparative study. AJR Am J Roentgenol. 2009 Oct;193(4):955-63. doi: 10.2214/AJR.08.2158.PMID: 19770316.
- Jeffrey RB Jr. CT angiography of the abdominal and thoracic aorta. Semin Ultrasound CT MR.1998 Oct;19(5):405-12. doi: 10.1016/s0887-2171(98)90017-8. PMID: 9800250.
- Ko JP, Goldstein JM, Latson LA Jr, Azour L, Gozansky EK, Moore W, Patel S, Hutchinson B. Chest CT Angiography for Acute Aortic Pathologic Conditions: Pearls and Pitfalls.Radiographics. 2021 Mar-Apr;41(2):399-424. doi: 10.1148/rg.2021200055. PMID: 33646903.
- Romanyukha, A., Nzitunga, P. S., & Dolcet, A. (2022, April 28). CT patient positioning plays key role in radiation dose reduction.www.auntminnie.com.
- Nienaber, C. A., Richartz, B. M., Rehders, T., Ince, H., & Petzsch, M. (2004). Aortic intramural haematoma:natural history and predictive factors for complications. Heart (British Cardiac Society), 90(4), 372–374.https://doi.org/10.1136/hrt.2003.027615
- Di Cesare, E., Splendiani, A., Barile, A., Squillaci, E., Di Cesare, A., Brunese, L., & Masciocchi, C. (2016). CT and MR imaging of the thoracic aorta.Open medicine (Warsaw, Poland), 11(1), 143–151. https://doi.org/10.1515/med-2016-0028
- Reginelli A, Capasso R, Ciccone V, Croce MR, Di Grezia G, Carbone M, Maggialetti N, Barile A, Fonio P, Scialpi M, Brunese L. Usefulness of triphasic CT aortic angiography in acute and surveillance: Our experience in the assessment of acute aortic dissection and endoleak.Int J Surg. 2016 Sep;33 Suppl 1:S76-84. doi: 10.1016/j.ijsu.2016.05.048. Epub 2016 May 29. PMID: 27250693.