CT Angio Circle of Willis (COW)
Last updated June 27, 2026
By Radiohelp Staff
Similar expressions
Brain CTA/ CT cerebral angio/ CT cerebral angiography/ CT COW angiogram
Introduction
CT COW is a contrast study, which helps to visualize cerebral arteries. It is used for the diagnosis of stroke, arteriovenous malformation (AVM), aneurisms and congenital abnormalities.
Patient preparation
- Explain the procedure clearly and kindly.
- Prepare the patient for contrast media administration.
- Place a ‘green cannula’ (18 G) in a stable vein with the ability of administering intravenous (IV) contrast media at a higher rate.
Patient positioning
- Secure the head with an immobilizing strap.
- Position the patient in head first supine and head on the head rest.
- Position patient's hands beside the body.
- Hand, which is used to infuse contrast media, is placed straight to facilitates the contrast flow.
- Center the scanning area in the scanner iso-center.
Explanation: this reduces overall radiation exposure and increases image quality [1].
Scan planning
There are two major techniques.
Method 1 - post-contrast single acquisition
- Plan the scan slab to cover from skull base to skull vertex.
- Plan the scan-and-view (S & V) slab just above the skull base.
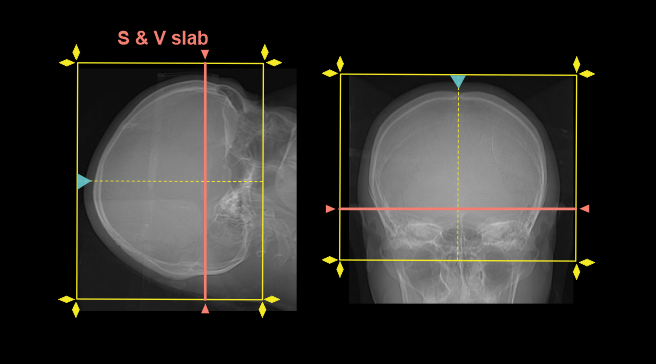
- Manual start is used to initiate the scan because it is quite challenging to find cerebral arteries in the S & V (pre-contrast) and also to place a small region of interest (ROI).
- Scan direction is planned to initiate from vertex to skull base.
Explanation: this avoids vertex delayed acquisition, visualizing cerebral veins.
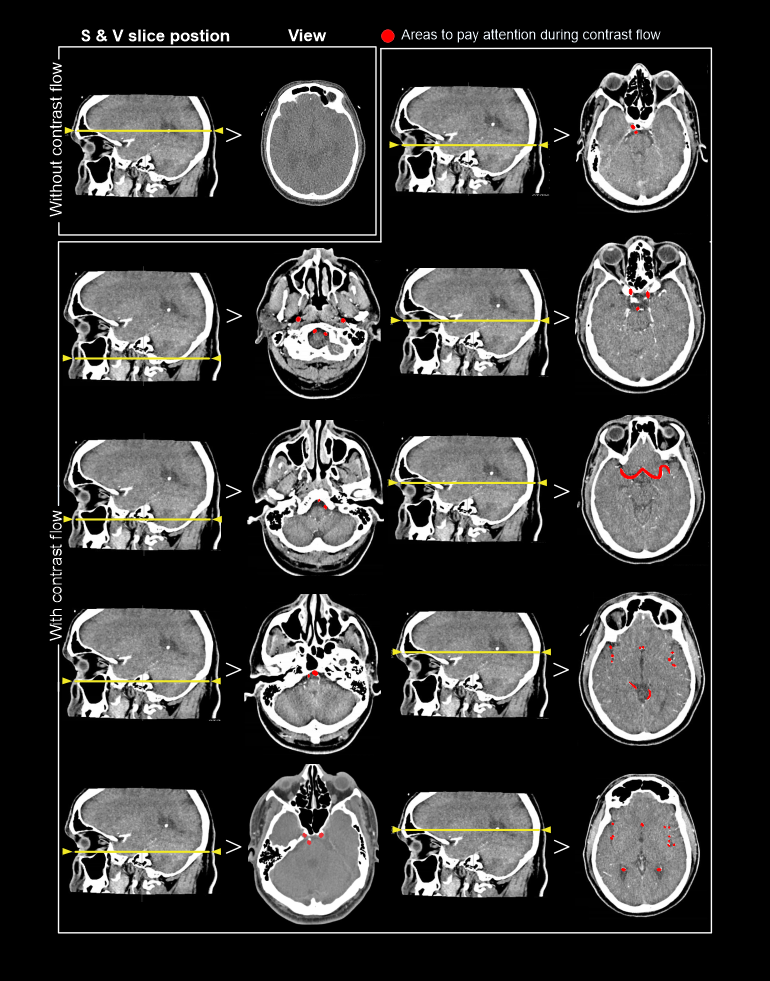
- Plan six seconds from contrast media initiation to S & V initiation.
- Plan minimum possible or zero delay time to start arterial scan.
Scan is manually started, when there is adequate amount of arterial opacification in the S & V image.
Method 2 - pre and post contrast for digital subtraction
- Plan both pre and post-contrast scan slabs to cover from skull base to skull vertex.
Explanation: parameters of start and end points of those slabs should be ideal, and patient should not move during both acquisitions , which are very important to make a successful digital subtraction.
- Plan the S & V slab just above the skull base.
- Manual start is used to initiate the scan.
- In the post contrast scan slab, scan direction is planned to initiate from vertex to skull base.
- Plan six seconds from contrast media initiation to scan-and-view initiation.
- Plan minimum or zero delay time to start arterial scan.
Contrast media administration
- 50ml to 60ml contrast volume can be used with a minimum flow rate of 4ml/s (for a 50-60kg body weight).
Explanation: higher flow rates are used in angiography to increase the vascular visualization.
- Start arterial scan immediately when there is slight enhancement in basilar or internal carotid arteries-in the S & V image.
When compare these two methods, post-processing is easy in the second method due to the digital subtraction, which is done by subtracting post-contrast data from pre-contrast data, leaving only the arteries in subtracted image. First method, however, has only arterial scan with lower radiation exposure, and it can be recommended for pediatric patients. Find more details about digital subtraction in our neck angiography article.
Post-processing
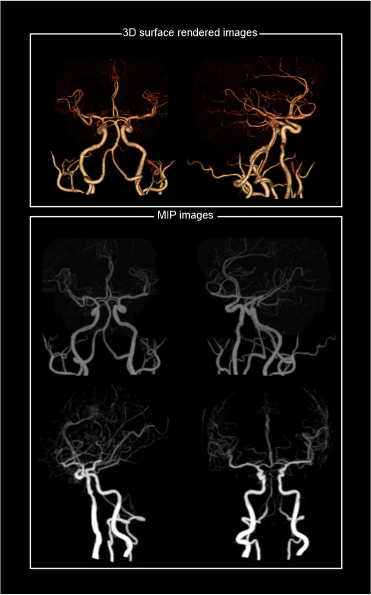
- Shaded 3D and Maximum intensity projection (MIP) images with a viewing angle of 360 degree.
- 2D images, in soft tissue window (ww:400 WL:40), in axial, coronal and sagittal planes, with a 2-3 mm slice thickness (reach brain contrast article to see images).
Reference
- Romanyukha, A., Nzitunga, P. S., & Dolcet, A. (2022, April 28). CT patient positioning plays key role in radiation dose reduction.
- Wintermark, MD, M., Blumfield, E., & E. Jordan, J. (2022). ACR–ASNR–SPR Practice parameter for the performance of computed tomography (CT) in the evaluation and classification of traumatic brain injury.
- Chen, Y., Manness, W., & Kattner, K. (2004). Application of CT angiography of complex cerebrovascular lesions during surgical decision making. Skull base: official journal of North American Skull Base Society ... [et al.], 14(4), 185–193.
- Heit, J. J., Pastena, G. T., Nogueira, R. G., Yoo, A. J., Leslie-Mazwi, T. M., Hirsch, J. A., &Rabinov, J. D. (2016). Cerebral Angiography for Evaluation of Patients with CT Angiogram-Negative Subarachnoid Hemorrhage: An 11-Year Experience. AJNR. American journal of neuroradiology, 37(2), 297–304.
- Fu F, Shan Y, Yang G, Zheng C, Zhang M, Rong D, Wang X, Lu J. Deep Learning for Head and Neck CT Angiography: Stenosis and Plaque Classification. Radiology. 2023 May;307(3): e220996. doi: 10.1148/radiol.220996. Epub 2023 Mar 7. PMID: 36880944.
- Hotta K, Sorimachi T,Osada T, Baba T, Inoue G, Atsumi H, Ishizaka H, Matsuda M, Hayashi N, Matsumae M. Risks and benefits of CT angiography in spontaneous intracerebral hemorrhage.Acta Neurochir (Wien). 2014 May;156(5):911-7. doi: 10.1007/s00701-014-2019-7.Epub 2014 Mar 7. PMID: 24604136; PMCID: PMC3988523.