Neck Angio CT
Last updated June 27, 2026
By Radiohelp Staff
Similar expressions
Neck CTA/ CT neck angio/ CT neck angiography/ CT neck angio with COW/ head and neck angio/ CTA carotids/ arch to vertex angiogram/ CT neck vessels/ Cervicocerebral CTA
Introduction
CTA carotids is a contrast study which helps to visualize carotid arteries and cerebral arteries. It is used for the diagnosis of stroke, arteriovenous malformation (AVM), aneurisms and congenital abnormalities. Anatomical coverage may vary with the patient’s condition, but usually it’s covered from the aortic arch to the skull vertex. In some instances to limit radiation exposure, scan is restricted to the head, performing cerebral angiography.
Patient preparation
- Explain the procedure clearly and kindly.
- Assess the ability to administer contrast media and expose radiation.
- Place a ‘green cannula’ (18G) in a stable vein with the ability of administering intravenous (IV) contrast media at a higher rate.
Patient positioning
- Position in head-first and supine.
- Position the head in the headrest and use immobilizing straps to secure it.
- Place the shoulders in a pulled down position and arms next to the body.
Explanation: reduces streak artifacts or beam hardening artifacts due to wide shoulders. Placing a cushion under mid-upper thorax moves shoulders posteriorly, and helps to reduce streak artifacts at the root of the neck [2].
- Ask not to move or swallow during the procedure.
- Hand, which is used to infuse contrast media, is placed straight to facilitate the contrast flow.
- Center the scanning area in the scanner iso-center [5].
Explanation: this reduces overall radiation exposure and increases image quality.
- Plan the scout starting point at the nipple level.
Scan planning
There are two major techniques.
Method 1 - Single, arterial scan.
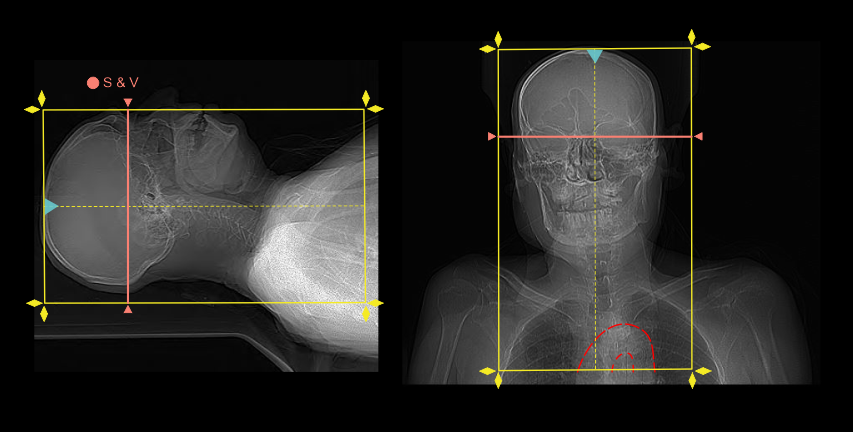
- Plan the scan slab to cover from vertex to aortic arch.
- Plan the scan-and-view (S & V) slab just above the skull base.
Explanation: manual start is used to initiate the scan because it’s quite challenging to find cerebral arteries in the scan-and-view slab (pre-contrast) and also to place a smaller region of interest (ROI).
- Scan direction is planned to initiate from head to foot.
Explanation: avoids delayed acquisition in superior region of the cerebral arteries, visualizing cerebral veins and evades streak artifacts at the root of the neck when there is undiluted contrast media in brachiocephalic and subclavian veins.
- Plan five seconds from contrast media initiation to S & V initiation.
- Plan zero or minimum delay time to start arterial step.
Method 2 - pre and post contrast dual scan for subtraction
- Plan pre and post contrast scan slabs to cover from vertex to aortic arch.
Explanation: parameters of start and end points of those slabs should be ideal, and patient should not move during both acquisitions , which are very important to make a successful subtraction.
- Phase initiation and planning is similar to the first method.
Intra venous (IV) contrast administration
- Contrast volume of 60ml can be used with a 4 to 4.5 ml/s flow rate – for a patient with 60-70kg body weight.
Explanation: higher flow rates are used in angiography to increase radio opaqueness of blood vessels.
- Arterial phase is started immediately when there is adequate contrast enhancement in basilar or internal carotid arteries (S & V image) – reach our neck contrast and cerebral angiography articles for images.
An additional step to capture venous phase can also be added to this scan – refer to our neck contrast article for more information.
Post-processing
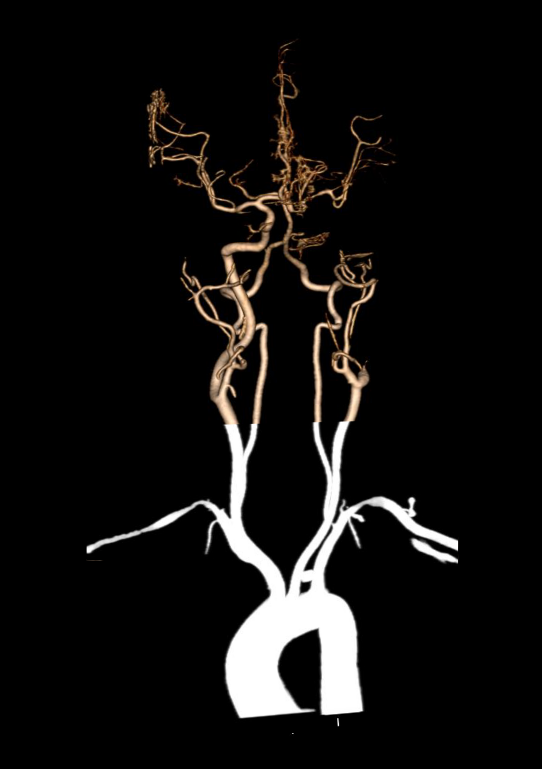
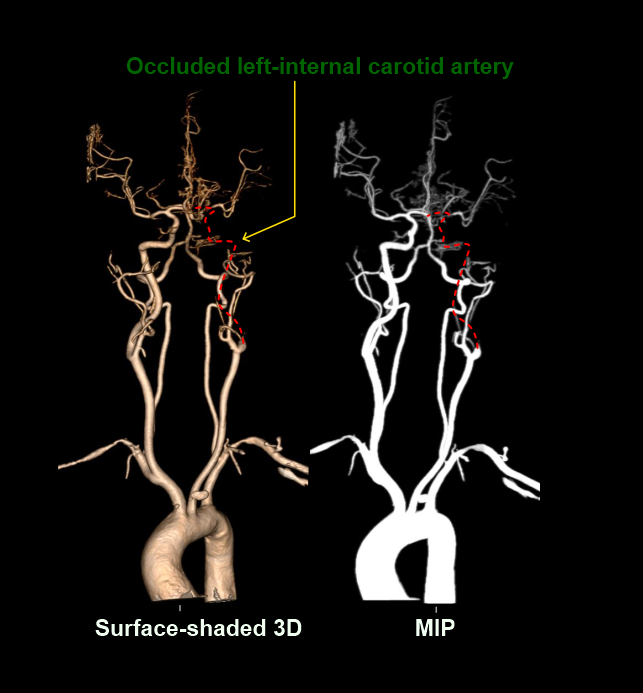
- Images in shaded 3D and maximum intensity projection (MIP) with a viewing angle of 360 degree.
- Axial, coronal and sagittal images in soft-tissue window (WW: 400, WL:40), without exceeding 3mm slice thickness – refer neck contrast article for images.
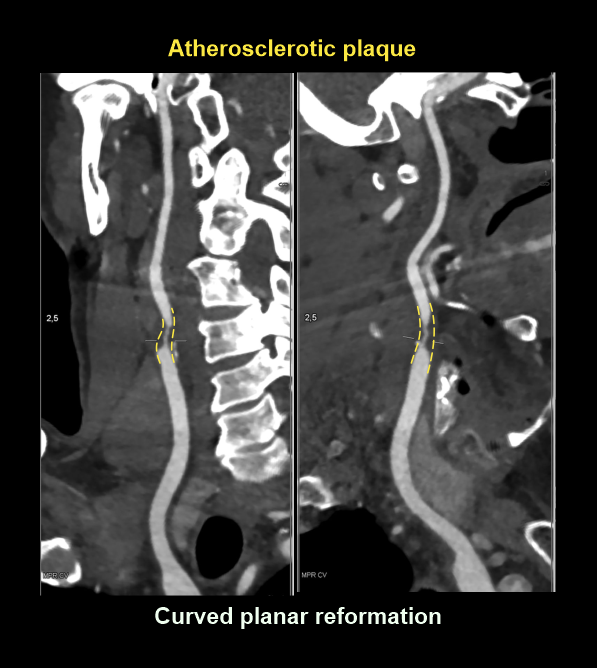
- Curved MPR images of arteries to clearly visualize atherosclerotic plaques.
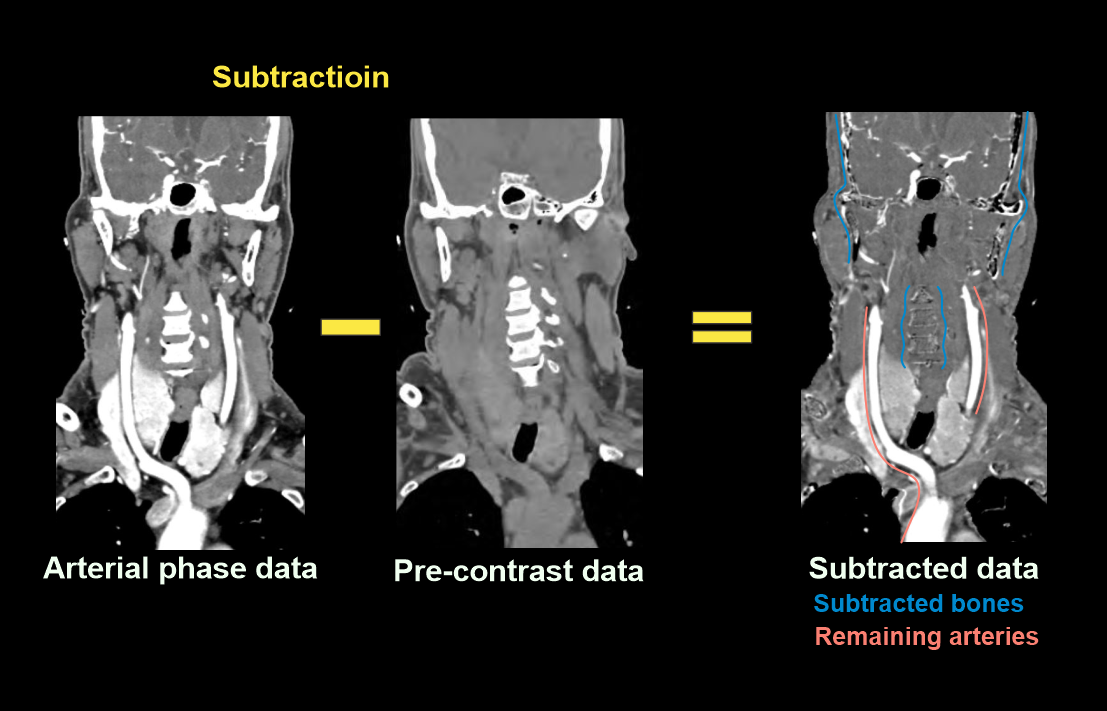
Subtraction eases post processing and provides crisp images. However, radiation dose for the patient is higher due to multiple acquisitions (pre and post contrast). So, this is not encouraged to use for pediatric patients.
Explanation: Subtraction is achieved by subtracting the scan data of post-contrast from pre-contrast. The main difference of these data sets is the contrast filled cerebral arteries, and it is the only thing that remains after subtraction.
Reference
- Alexander M. McKinney, IV, MD, Co-Chair, Max Wintermark, MD, Co-Chair, & Amanda S. Corey, MD, FACR. (2020). ACR–ASNR–SPR Practice parameter for the performance and interpretation of cervicocerebral Computed Tomography angiography (CTA).Retrieved from www.gravitas.acr.org.
- Harvey, G. D., Mayer, D. P., & Radecki, P. D. (1984). Simplified patient positioning to reduce beam hardening in CT of the lower neck. AJNR. American journal of neuroradiology, 5(6), 796.
- Zhang, W. L., Li, M., Zhang, B., Geng, H. Y., Liang, Y. Q., Xu, K., & Li, S. B. (2013). CT angiography of the head-and-neck vessels acquired with low tube voltage, low iodine, and iterative image reconstruction: clinical evaluation of radiation dose and image quality.PloS one, 8(12), e81486. https://doi.org/10.1371/journal.pone.0081486.
- Ma, G., Yu, Y., Duan, H., Dou, Y., Jia, Y., Zhang, X., Yang, C., Chen, X., Han, D., Guo, C., & He, T. (2018). Subtraction CT angiography in head and neck with low radiation and contrast dose dual-energy spectral CT using rapid kV-switching technique.The British journal of radiology, 91(1086), 20170631. https://doi.org/10.1259/bjr.20170631.
- Romanyukha, A., Nzitunga, P. S., & Dolcet, A. (2022, April 28). CT patient positioning plays key role in radiation dose reduction.www.auntminnie.com.
- Schepers, Christophe & Schepers, Steven & Student, Medical & Ku, Leuven. (2016). Partial oculomotor nerve palsy due to a basilar tip aneurysm.. eurorad. 10.1594/EURORAD/CASE.13770.
- Eller, A., Wiesmüller, M., Wüst, W., Heiss, R., Kopp, M., Saake, M., Brand, M., Uder, M., & May, M. M. (2019). Carotid CTA at the Lowest Tube Voltage (70 kV) in Comparison with Automated Tube Voltage Adaption.AJNR. American journal of neuroradiology, 40(8), 1374–1382. https://doi.org/10.3174/ajnr.A6108