CT Colonoscopy
Last updated April 10, 2026
Similar expressions
CTC/ CT virtual colonoscopy/ CT virtual colonography/ CT colonography/ CT pneumocolon
Introduction
CT colonography is a minimally invasive procedure that can be used to diagnose colorectal cancer, and CTCis helpful for patients with narrow strictures where optical colonoscopy is challenging.
Patient preparation
- Explain the procedure clearly and kindly.
- Check the ability to expose radiation.
- Check allergic reactions for contrast media and laxatives.
- Assess patient history and routine medication.
- Remove metals related to the interested region.
Important: Avoid the procedure if the patient is having contraindications such as symptomatic acute colitis, acute diarrhea, recent acute diverticulitis, recent colorectal surgery, symptomatic colon-containing abdominal wall hernia, recent deep endoscopic biopsy or polypectomy/mucosectomy, known or suspected colonic perforation and symptomatic or high-grade small bowel obstruction. Moreover, CT Colon scan is not indicated for conditions such as routine follow-up of inflammatory bowel disease, hereditary polyposis or nonpolyposis cancer syndromes, evaluation of anal canal disease and the pregnant or potentially pregnant patient.
- Practice breath out and hold technique (end expiration).
Explanation: this is to minimize pressure on the transverse colon due to inflated lungs and avoidmotion artifacts.
- Prepare patient's bowel according to following steps.
Bowel preparation
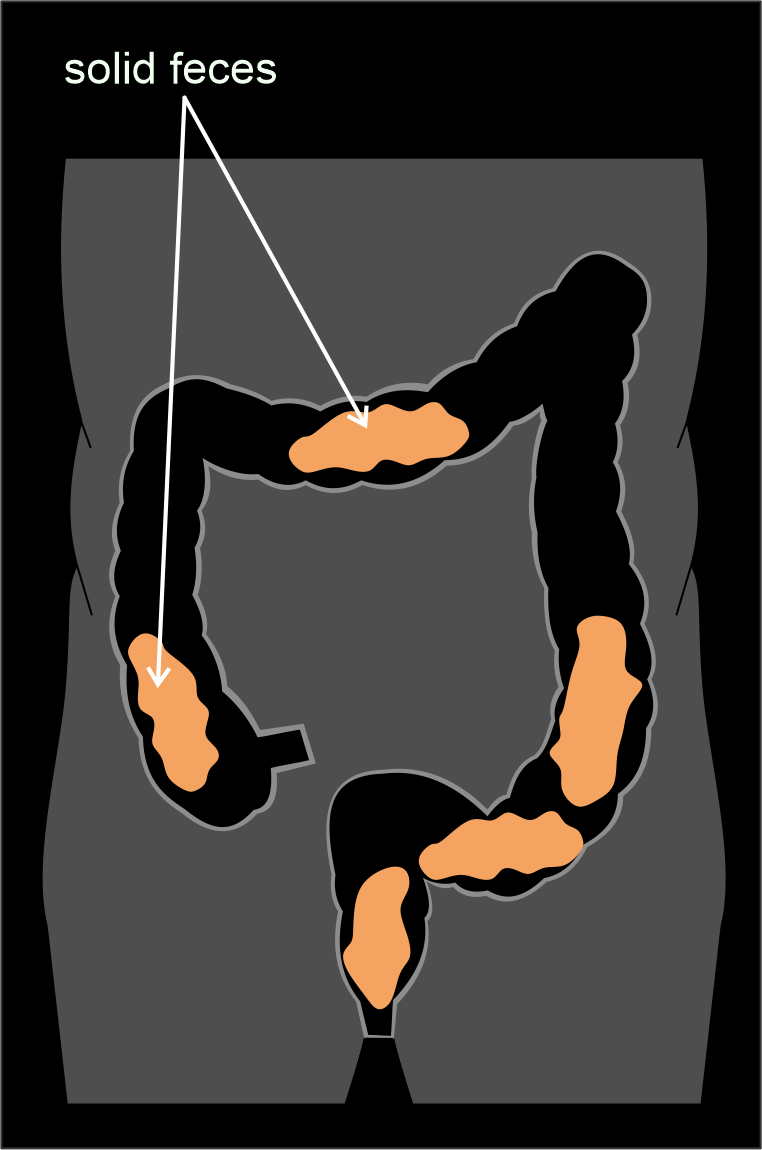
Bowel preparation is the most important part in CTC procedure because poor bowel preparation can increase the chance of misdiagnosis due to residual fecal matter and fluid. There are mainly two types of bowel preparation methods. In one method, fecal tagging agent is used and in the other it is avoided. However, both of them share basic steps including low residue diet, clear fluid intake and laxative intake.
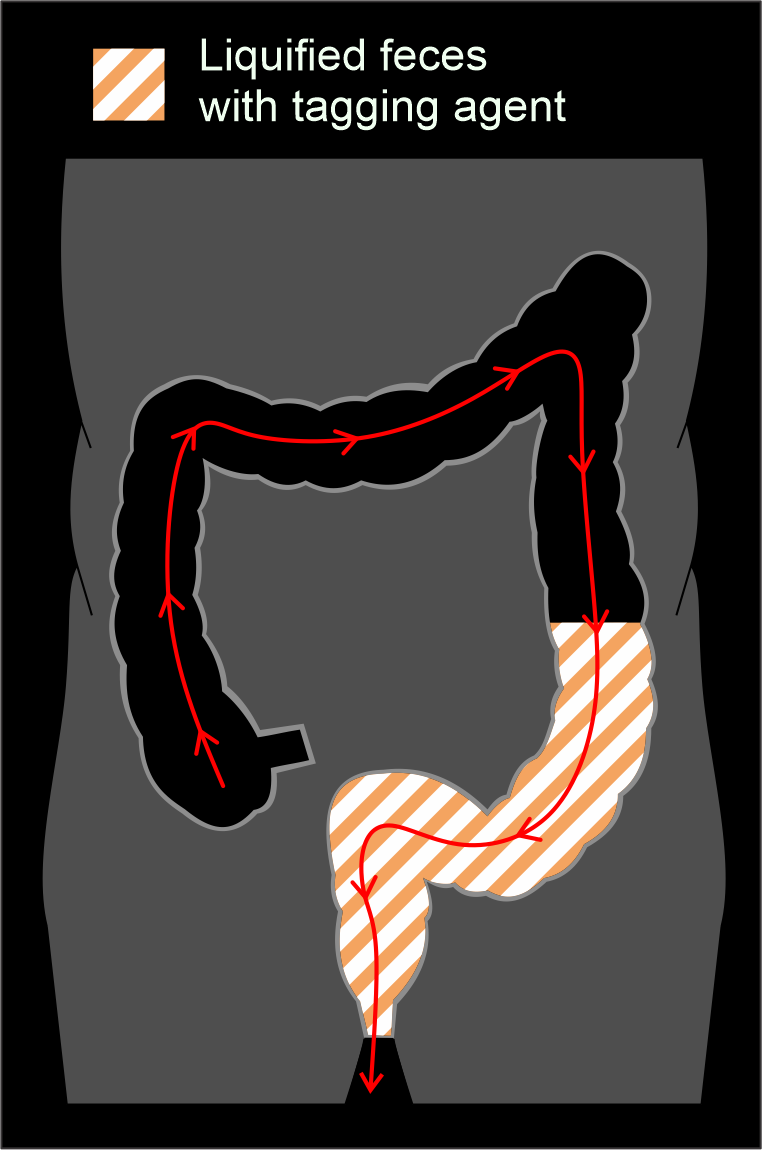
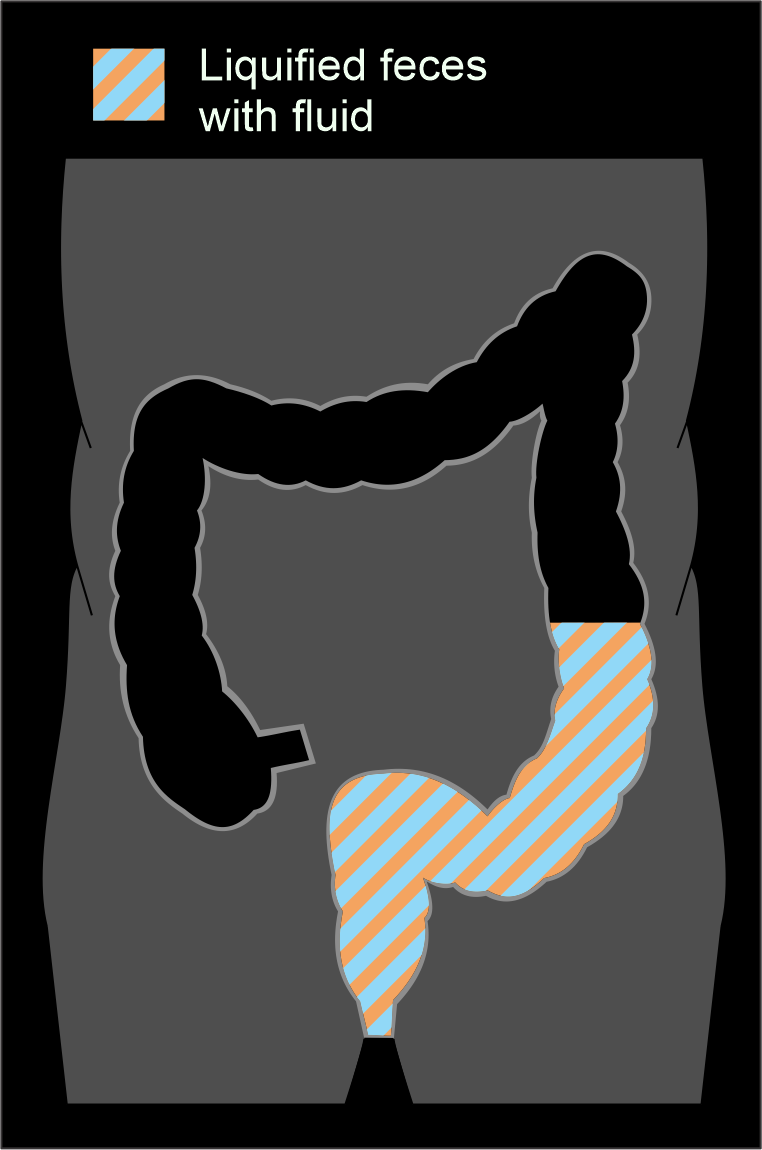
Method 1-Bowl preparation with fecal tagging agent (wet preparation)
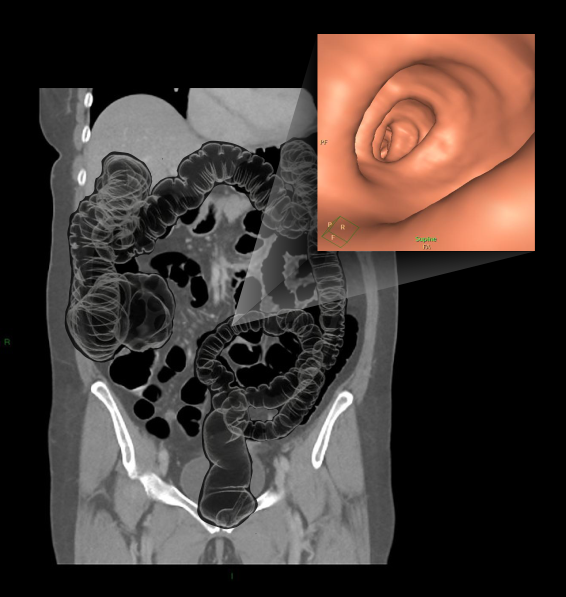
This method is different from the other due to Its use of oral-tagging agent. Mainly, there are two types of agents known as Gastrografin and Microcat, which contain iodine and barium respectively, and they act as a fecal tagging medium as well as a laxative. Usually, images are viewed as MPR because the residual contrast-fluid mixture may act as a barrier to view the bowel wall using 3D virtual fly through.
Method 1 preparatory steps:
7 Days before the appointment date
- Stop taking iron tablets and weight loss medication.
- Continue all regular medication – seek help from a medical officer for any doubts regarding medication withdrawal.
4 Days before
- Stop taking constipation medication.
- Continue all regular medication.
1 Day before
- Before 7am: Drink Gastrografin 1st portion, 1 hour before breakfast – mix 75 mls of Gastrografin with an equal amount of water. Cordial may be added.
- Before 8am: Take breakfast limited to boiled or poached egg and/or white bread with a scraping of butter or margarine.
- 12am to 1pm period: Take lunch limited to the following meals: a small portion of steamed, poached or grilled white fish or chicken; a small portion of boiled potatoes (2 eggs sized) or two slices of white bread; jelly for dessert (this may contain sugar).
- After lunch: no solid food until appointment. Clear fluids are allowed, but limited to tea, coffee, squash, water, clear fruit juices (grape, apple, cranberry) and fizzy drinks. Drink at least 150ml of fluid every hour during the day time.
- 7pm: Drink Gastrografin 2nd portion – mix 25 mls of Gastrografin with an equal amount of water. Cordial may be added.
- Do not eat or drink: Red meats, pink fish e.g. salmon; Fruit, vegetables, salad, mushrooms, sweetcorn; cereals, nuts, seeds, pips, bran, beans, lentils; Brown bread, brown or wild rice, brown pasta; Pickles or chutneys; Milk, thick soup, alcohol.
Day of the appointment
- No solid foods until after procedure. Clear fluids are allowed, but limited to tea, coffee, squash, water, clear fruit juices (grape, apple, cranberry) and fizzy drinks. Drink at least 150ml of fluid every hour during the day time.
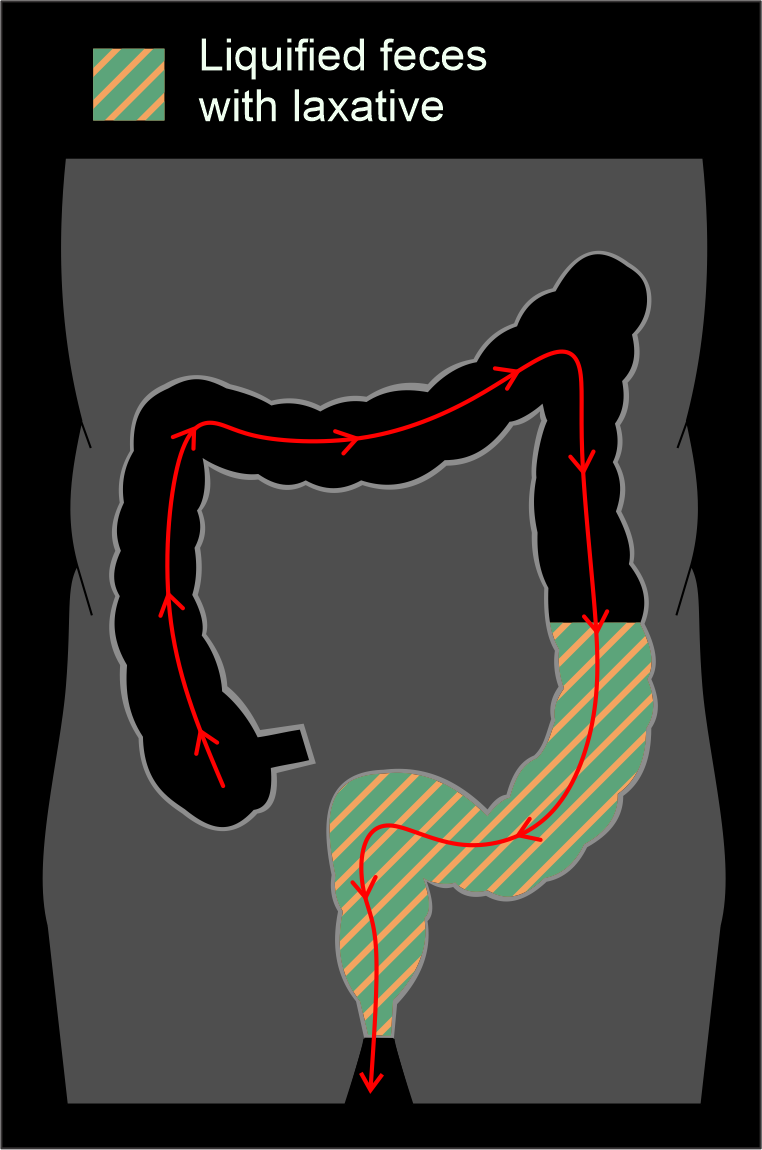
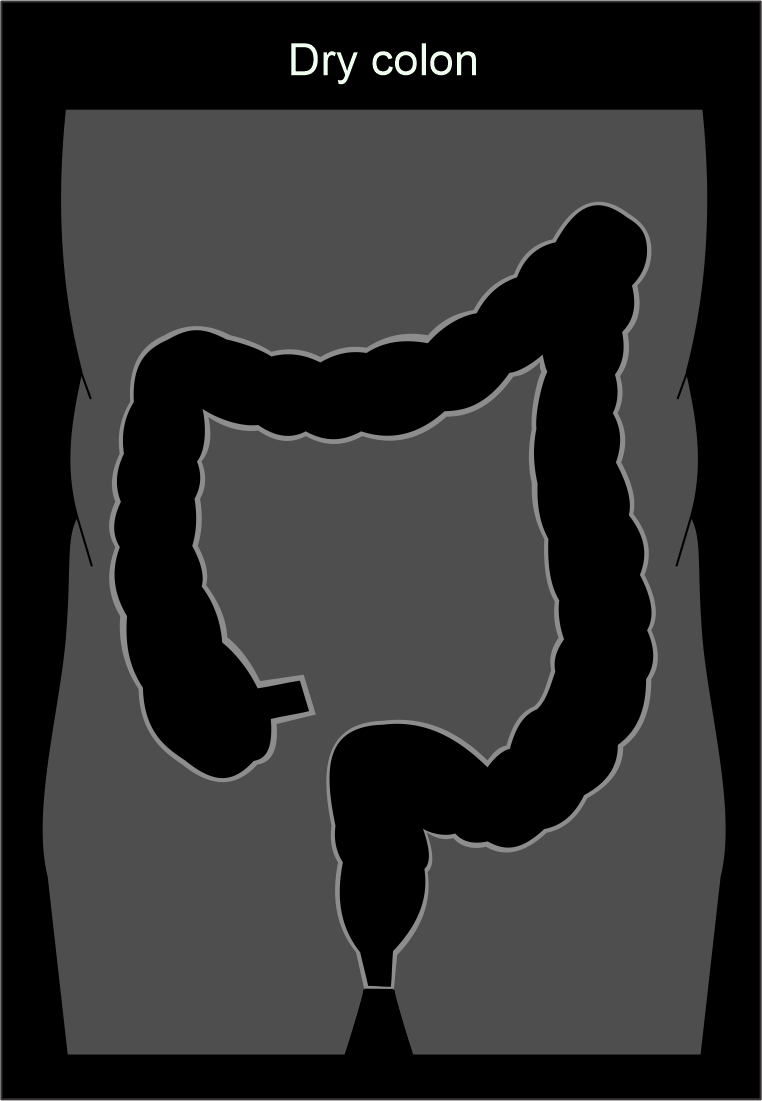
Method 2 - Bowl preparation with laxatives (dry preparation).
This method is ideal to the colon preparation for conventional colonoscopy. There is no any involvement of fecal tagging agents except fasting and laxatives, providing a dry colon free of fluid and feces, and 3D virtual fly through can be used here.
Method 2 preparatory steps:
7 Days before the appointment date
- Stop taking iron tablets and weight loss medication.
- Continue all regular medication – seek help from a medical officer for any doubts regarding medication withdrawal.
4 Days before
- Stop taking constipation medication.
- Continue all regular medication.
2 Days before
- For all breakfast, lunch and dinner, take a low residue diet and drink plenty of fluids (two liters a day) only limited to the following: Well cooked, lean (low fat) beef, lamb, ham, veal or pork; Fish, shellfish or poultry; White rice, noodles or white pasta; Cereal including cornflakes and crisped rice cereal, but not bran; White bread or toast; Rich tea or other plain biscuits; Eggs, especially boiled or poached; Butter, margarine or cheese; Milk, cream or cottage cheese; Potatoes without the skins (boiled, creamed, mashed or baked); Soya or tofu; Gravy made from stock cubes (you can use plain flour or cornflour to thicken this); Sugar or sweetener; Clear jelly; Water, cordial, fizzy drinks, clear strained soup or clear stock.
- Do not eat or drink: Fruit, including fresh, dried and canned; Brown rice or brown pasta; High-fibrebreakfast cereals (including porridge oats); Pulses or lentils; High-fibre, multi-seeded, 50/50 or wholemeal bread; Vegetables; Nuts or seeds; Roasted, deep fried potatoes (including chips); Crisps, jam, red jelly; Red cordial or fruit juice, alcohol.
1 Day before
- Before 9am: Take breakfast, but limited to following drinks and meals: eggs, white bread, toast, butter or margarine, croissants, shredless marmalade or jam; black tea or coffee water, fizzy drinks, fruit squash but not blackcurrant as this stains the bowel.
- After breakfast, for a morning appointment, don’t eat solid food until after CT colonography procedure. Patient can have lunch (from the meals and drinks above) at 1:00 pm for an afternoon appointment.
- Drink clear fluids only today limited to water, squash, fizzy drinks, clear strained soup and clear stock.
- Patient need to take multiple laxative sachets, and starting time may change according to the laxative type. There are numerus types of laxatives that can be used to clean colon such as Klean-Prep, Moviprep and Picolax or CitraFleet, and their usage are different. It is important to seek help from a pharmacist to know the correct method of preparation.
- 5pm: take the 1st laxative sachet. Drink this over 1 – 2 hours, which works within 2 hours. Patient need to stay close to a toilet as diarrhea effects start.
- 8:00 pm: take the 2nd laxative sachet as the 1st one.
On the day of the procedure
- Continue drinks or fluids from the allowed list until 2 hours before procedure and no solid food until after CT colonography.
Explanations:
Avoiding iron tablets
Taking iron tablets prior to the procedure may cause constipation, allowing dried feces to retain in the bowel. To avoid this, constipation causing medication should be avoided. Additionally, it may cause side effects such as nausea, vomiting, diarrhea and losing appetite, which may interrupt proper preparation.
Low residue diet.
A diet with fibers increases the chance of fecal residue in the colonic lumen that looks like polyps or pathologies. So, a low residue diet is more suitable to limit fecal residues.
Clear fluid intake.
This is very important for the patient to stay hydrated during preparatory period and wash out fecal residues from colon with its laxative effects.
Laxative intake.
Laxatives help to cleanse the bowel by increasing fluid retention in colon and promote bowel motion to excrete food residues.
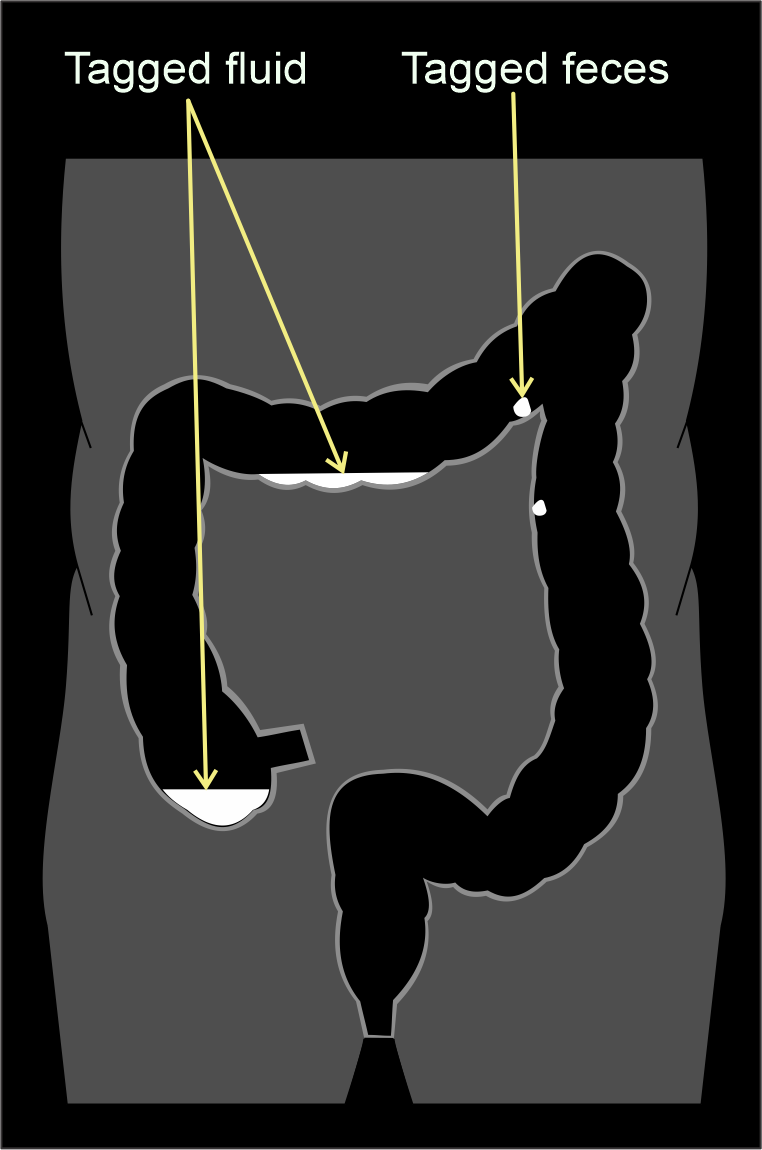
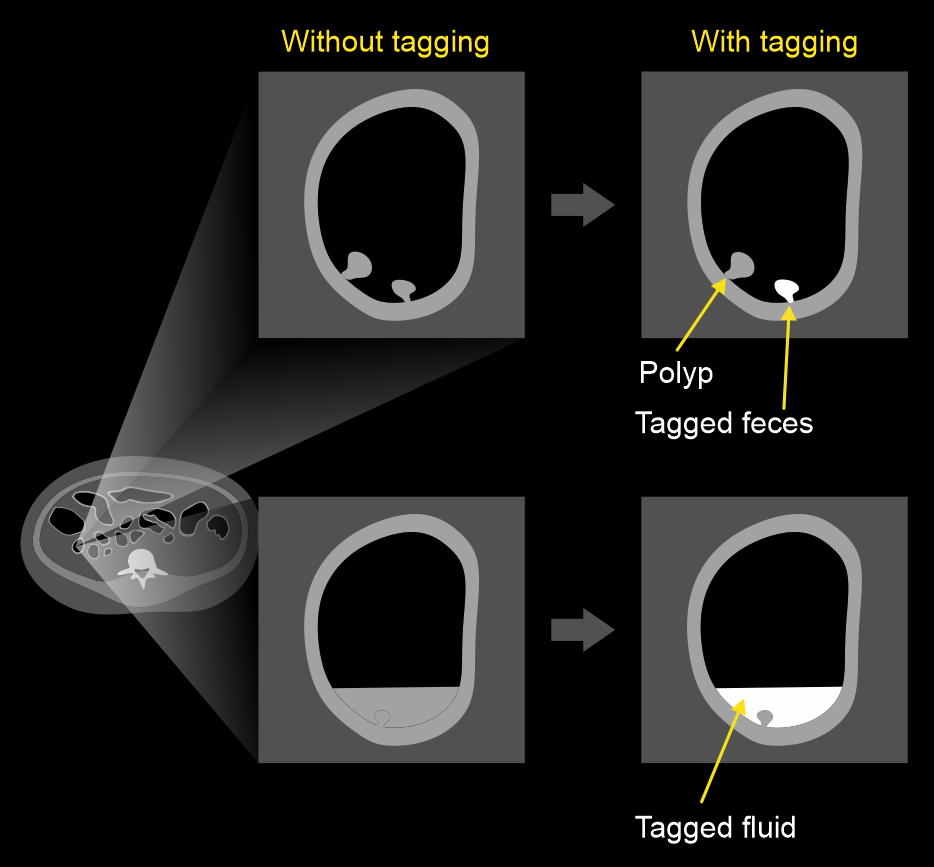
Fecal tagging.
Feces absorb radio-opaque iodine or barium or tagging agents, but polyps can’t directly absorb them. As a result, true polyps appear isodense when compared with the hyperdense feces. In addition, tagging agents dissolve in residual fluid in the colon, which appear hyper dense in images. So, these agents tag residual fecal matter as well as fluid, helping to differentiate true polyps.
Patient positioning
Colon insufflation need to be performed beforehand the scan.
Colon insufflation
Human colon has folds in the bowel lumen, which hides pathologies such as polyps and diverticula. Because of that, bowel wall has to be stretched like a balloon by introducing air in to the colon, and this helps to stretch the folds to simplify the lumen anatomy.
- Evacuate the patient before rectal tube insertion.
- Turn the patient in to left lateral decubitus (Sims) position with slightly flexed knees and hips and, gently place the rectal tube.
- Introduce Carbon dioxide in to the colon by mechanical insufflation (preferred method) or roomair by manual insufflation.
Explanation: colonic mucosa rapidly absorbs CO2 than room air, reducing discomfort after procedure.
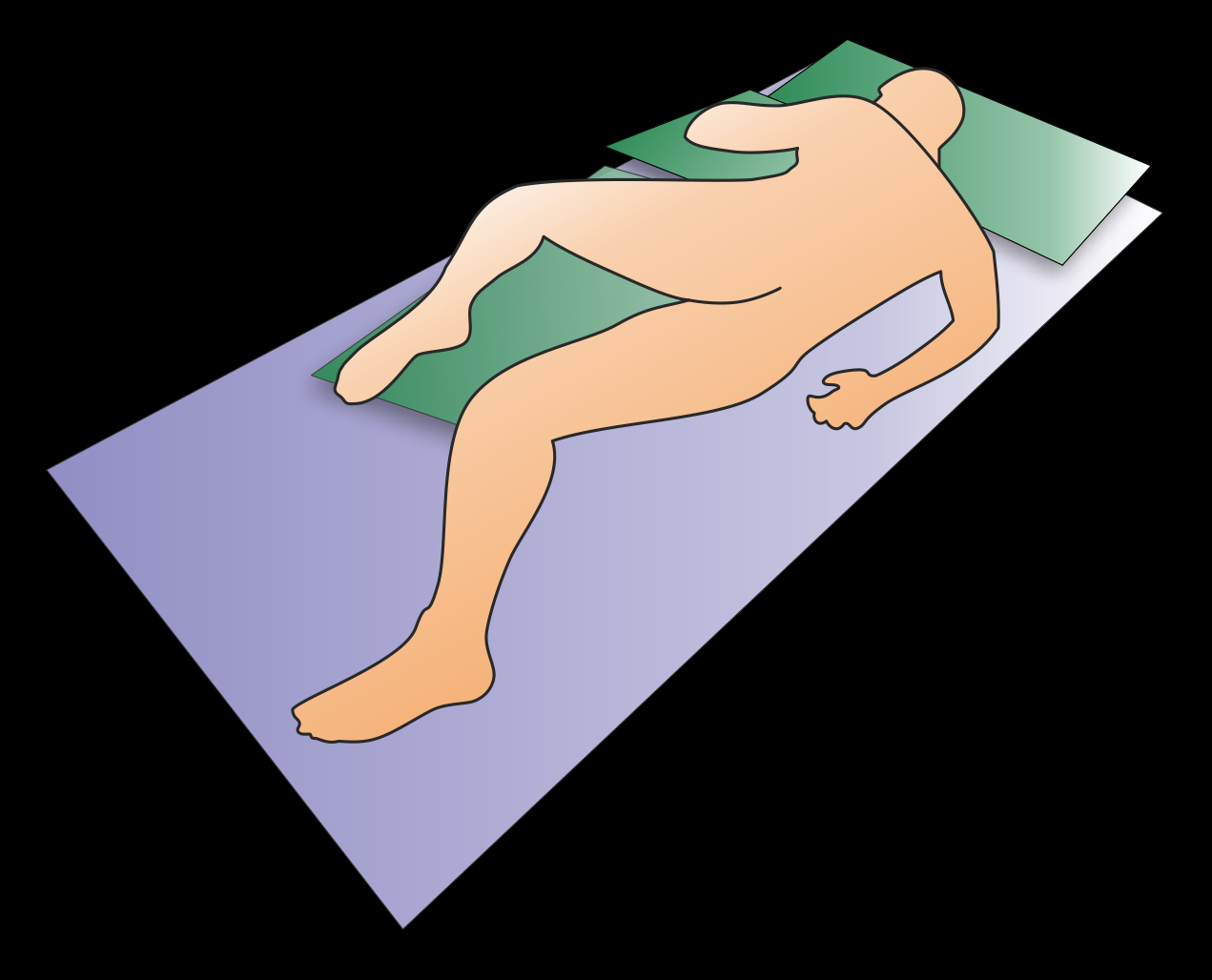
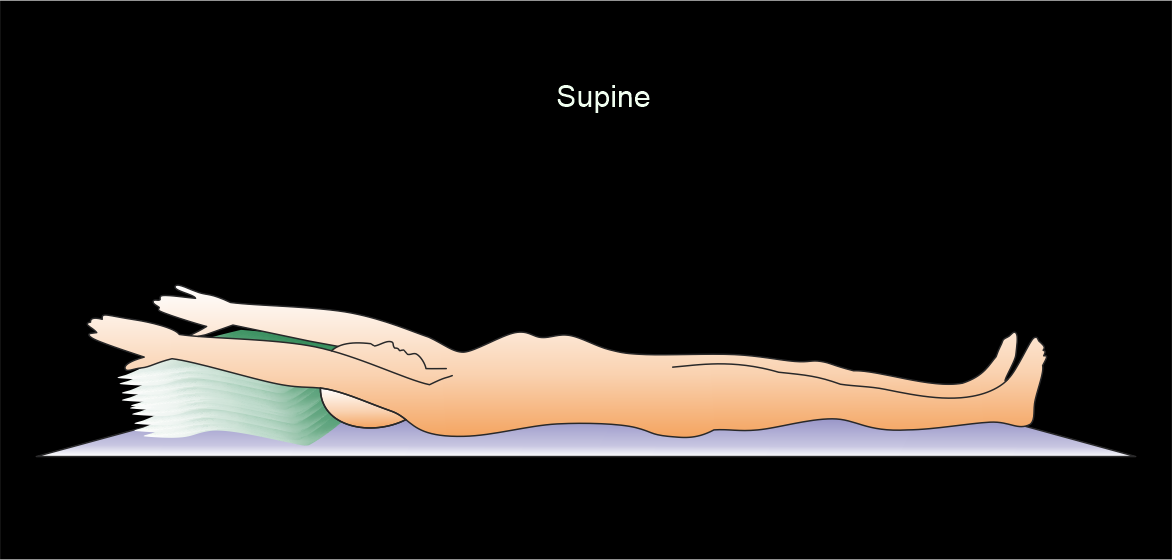
- Turn in to supine position after achieving a full colon distension, and perform a scout view toconfirm.

Scanning
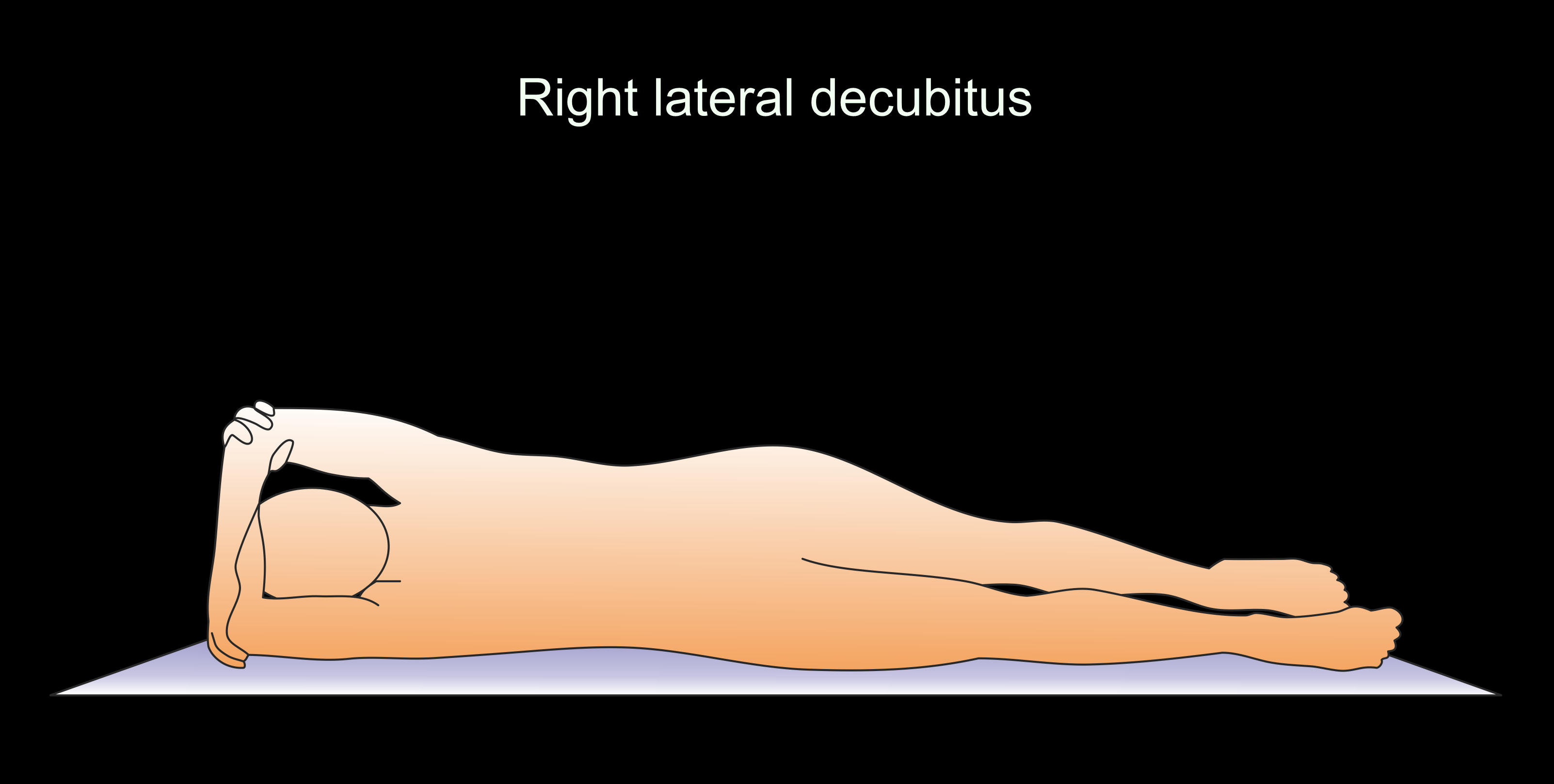
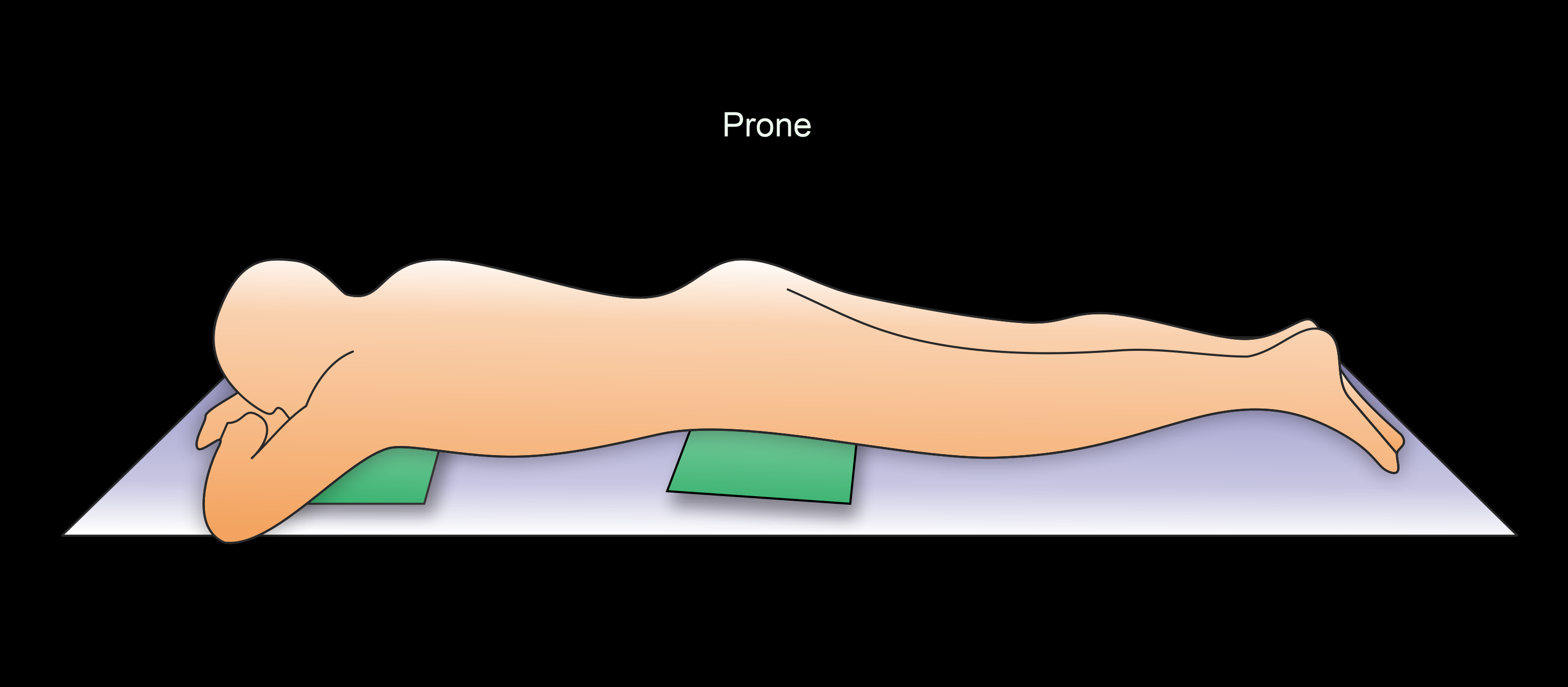
- Scan at least for 2 positions – supine and prone (common), supine and right lateral decubitus or bilateral decubitus.
Explanation: to view the colon luminal surface segments at least in one position, and differentiate mobile small fecal particles from stable true polyps.

- Place 2 pillows under the chest and the pelvis area for prone position.
Explanation: to avoid pressure on the transverse colon from the anterior wall of the abdomen.
- Refill scaping air when the patient switch positions.
If IV contrast is needed, perform a non-contrast prone scan followed by a series of supine post contrast scans as mentioned in the CT multiphase contrast abdomen scan.
- Center the scanning area in the scanner iso-center [6].
Explanation: this reduces overall radiation exposure and increases image quality.
- Refrain from allowing patient’s hands lying next to the abdominal area.
Explanation: this reduces streak artifacts from the hands, also it avoids unnecessary radiation exposure to the hands.
Scan planning
- Plan the scan slab to cover from the dome of the diaphragm to a level just below the ischial tuberosities.
Refer non-contrast abdomen scan for images.
Explanation: to completely cover both colon and rectum.
- Perform all scans under end expiration.
Refer CT multiphase contrast abdomen scan for post-contrast scan planning.
Post-processing
- MPR (axial, sagittal and coronal) views in soft-tissue window with 2mm slice thickness and 2mm gap for all patient positions (supine, prone and post contrast phases).
Refer non-contrast abdomen scan for images.
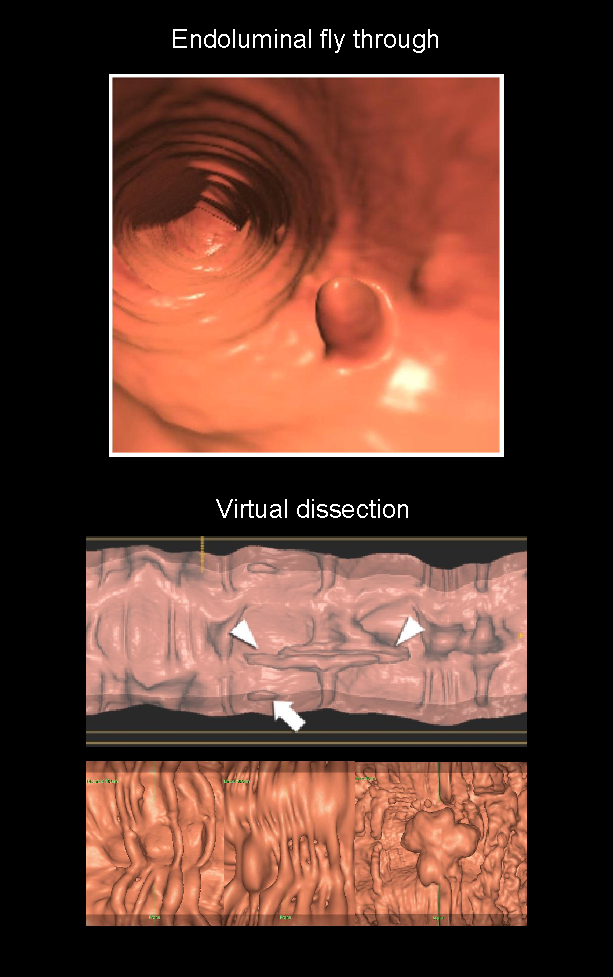
- 3D endoluminal fly-through view.
- Alternative 3D display views such as virtual dissection.
Reference
- Taylor, S. A., Slater, A., Burling, D. N., Tam, E., Greenhalgh, R., Gartner, L., Scarth, J., Pearce, R., Bassett, P., & Halligan, S. (2008). CT colonography: optimisation, diagnostic performance and patient acceptability of reduced-laxative regimens using barium-based faecal tagging. European radiology, 18(1), 32–42. https://doi.org/10.1007/s00330-007-0631-0
- Nagata K, Singh AK, Sangwaiya MJ, Näppi J, Zalis ME, Cai W, Yoshida H. Comparative evaluation of the fecal-tagging quality in CT colonography: barium vs. iodinated oral contrast agent.Acad Radiol. 2009 Nov;16(11):1393-9. doi: 10.1016/j.acra.2009.05.003. Epub 2009 Jul 10. PMID: 19596591.
- Park SH, Yee J, Kim SH, Kim YH.Fundamental elements for successful performance of CT colonography (virtual colonoscopy). Korean J Radiol. 2007 Jul-Aug;8(4):264-75. doi: 10.3348/kjr.2007.8.4.264. PMID: 17673837; PMCID: PMC2627155.
- Yee, Judy MD, Chair, Brewington, Cecelia Cody MD, Dachman, Abraham MD, & Dane, Bari MD. (2024). ACR–SABI–SAR Practice parameter for the performance of computed tomography (CT) colonography in adult. Retrieved from www.gravitas.acr.org.
- Pickhardt, P. J., & Kim, D. H. (2013). CT colonography: pitfalls in interpretation. Radiologic clinics of North America, 51(1), 69–88. https://doi.org/10.1016/j.rcl.2012.09.005
- Romanyukha, A., Nzitunga, P. S., & Dolcet, A. (2022, April 28). CT patient positioning plays key role in radiation dose reduction.www.auntminnie.com.
- Lefere, P., & Gryspeerdt, S. (2011). CT colonography: avoiding traps and pitfalls.Insights into imaging, 2(1), 57–68. https://doi.org/10.1007/s13244-010-0054-3
- Mang, T., Bräuer, C., Gryspeerdt, S., Scharitzer, M., Ringl, H., & Lefere, P. (2020). Electronic cleansing of tagged residue in CT colonography: what radiologists need to know.Insights into imaging, 11(1), 47. https://doi.org/10.1186/s13244-020-00848-9