CT Urogram
Last updated April 14, 2026

Similar expressions
CT urogram/ CTIVU/ CTIVP/ CTU scan/ CT intravenous pyelography/ CT IVP/ CT IVU
Introduction
Usually, CTIVU is requested for patients who are detected with blood in urine (hematuria). Study can be used to diagnose renal stones, strictures and renal neoplasms.
Patient preparation
- Explain the procedure clearly and kindly.
- Check contraindications for contrast media administration and radiation exposure.
- Remove metals related to the interested region.
- Place an Intra venous (IV) cannula in a stable vein of an arm – green-18G cannula.
Explanation: green cannula has higher lumen diameter, which can withstand higher flow rate.
- Provide 1000ml of water to drink within 20-30min without emptying the urinary bladder.
Explanation: this is to adequately fill the bladder with urine, which promotes visualization of ureters.
- Start the scan when the patient’s having a fully filled bladder.
Patient positioning
- Position the patient in supine and feet first on the imaging couch.
- Center the scanning area in the scanner iso-center [6].
Explanation: this reduces overall radiation exposure and increases image quality.
- Raise both hands above the head and place a positioning aide under them.
Explanation: hands beside the trunk give streak artifacts and increase radiation exposure.
- Keep the arm with the IV cannula strait.
Explanation: to facilitate contrast flow.
- Plan the scan starting point at the nipple level.
Scan planning
Pre-contrast and post-contrast steps are mandatory for this scan, but more steps may be added depending on the diagnostic needs of the patient.
Two step method simply can be used to diagnose stenosis in the ureters, but without suspectedneoplasms.
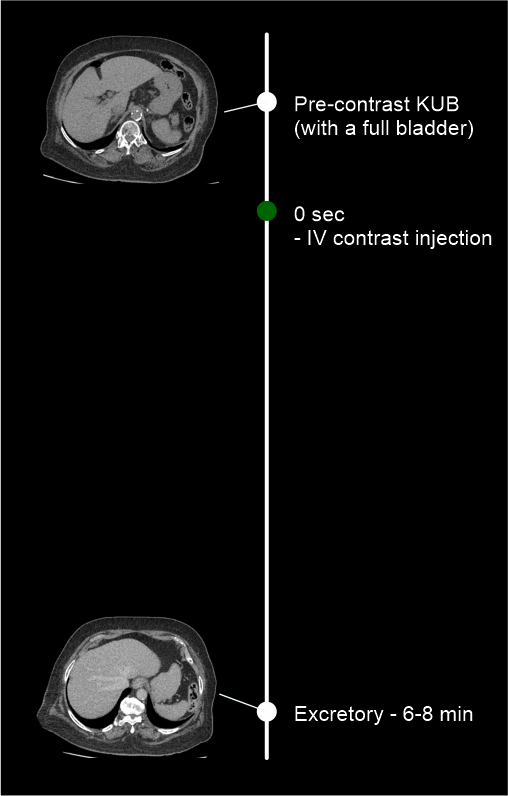
- Use time-bolus method for phase initiation – refer CT multiphase abdomen scan for more details.
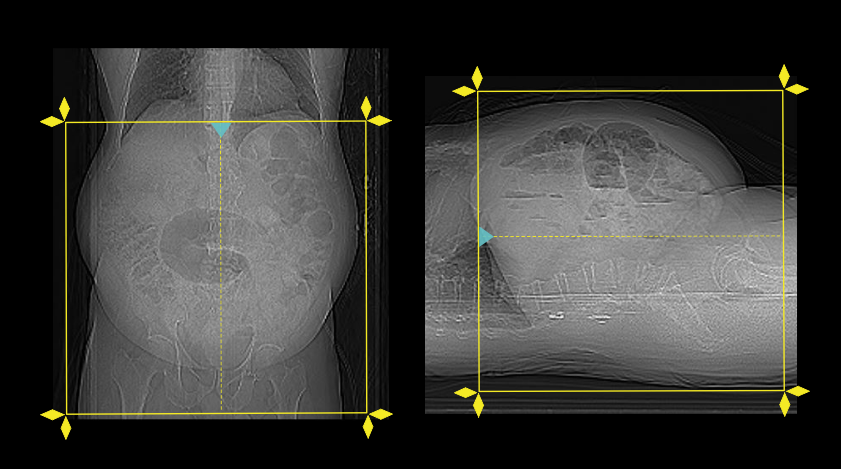
- Plan both pre-contrast and excretory phases to cover from dome of the diaphragm to a level just below the ischial tuberosities.
Four step method is more suitable for patients with renal neoplasms.
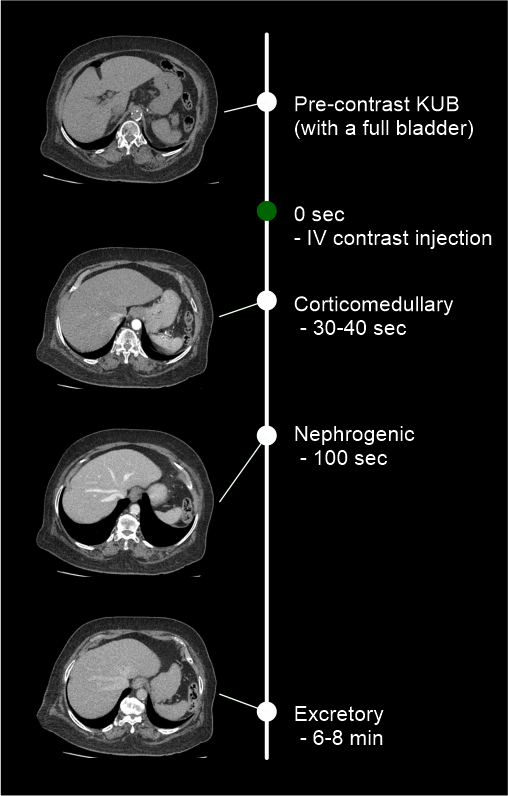
- Use bolus-tracking method for phase initiation – reach CT multiphase abdomen scan for more information.
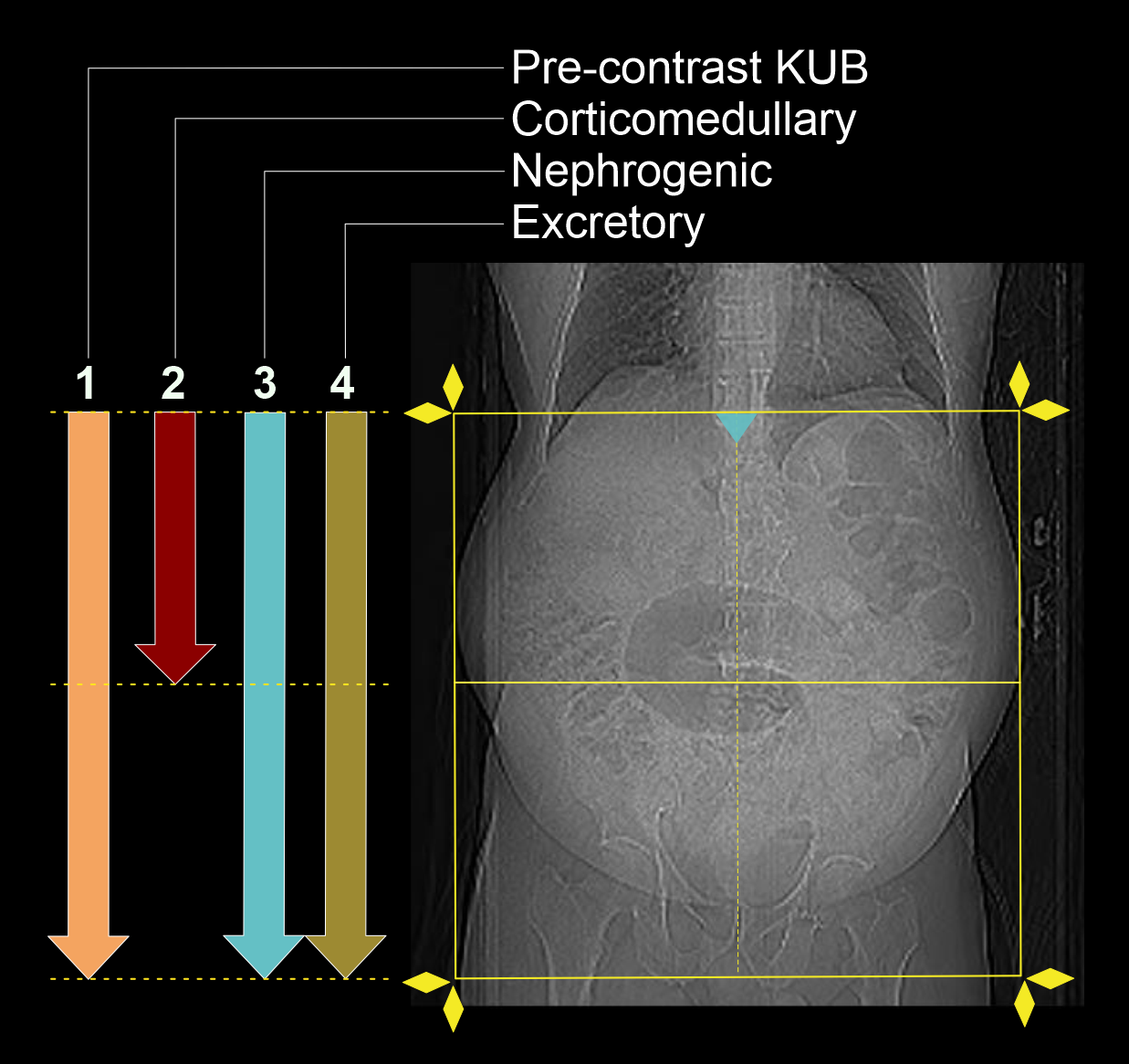
- Plan all pre-contrast, nephrogenic and excretory phases to cover from the mid-diaphram to a level below the ischial tuberosities.
- Plan corticomedullary phase to cover from the mid-diaphragm to the iliac crest.
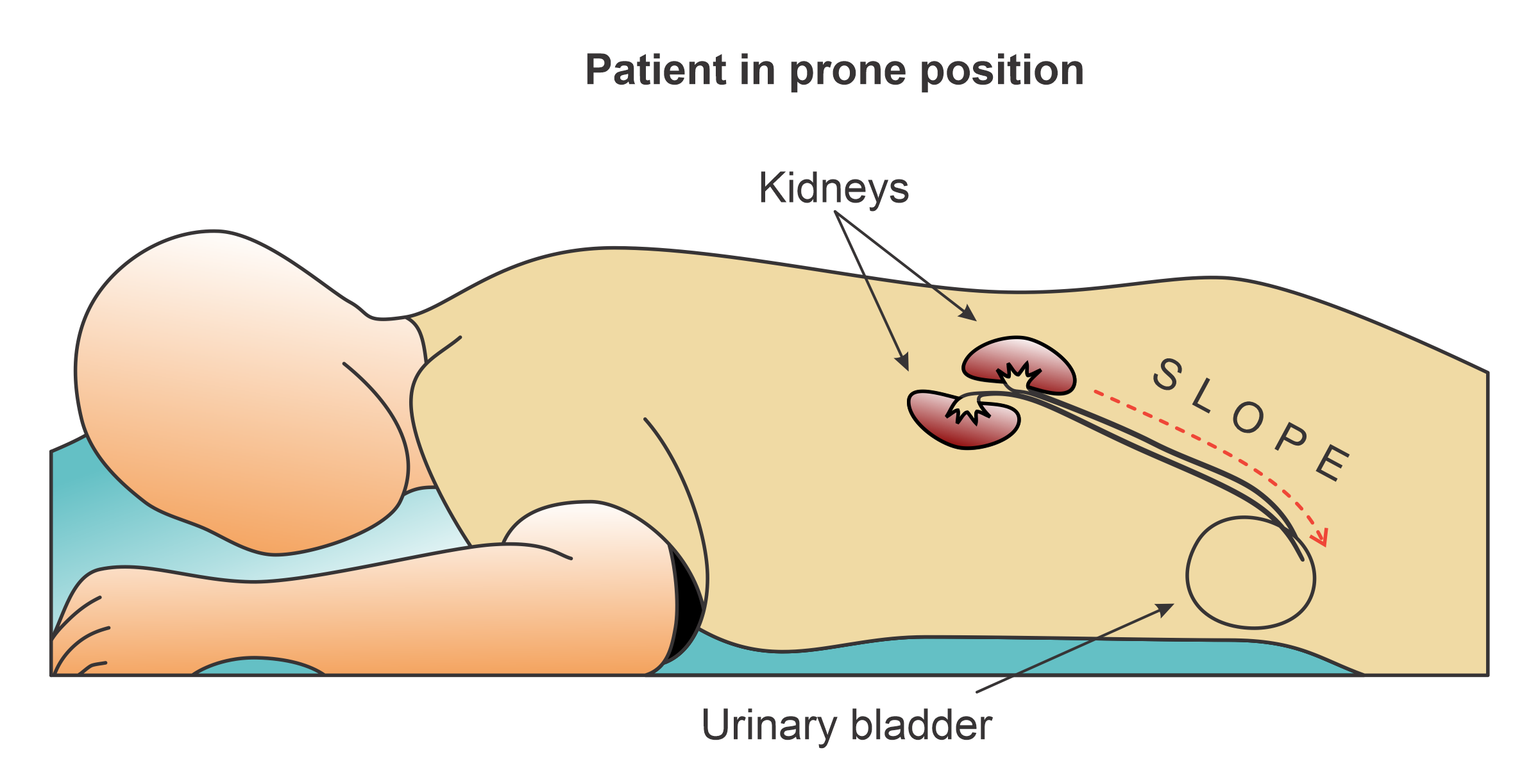
In excretory phase, you can promote contrast flow into the distal part of ureters by scanning the patient in prone position because a slope is created from kidneys to bladder.
Intravenous (IV) contrast infusion
- For two step method, inject 80 ml (for a patient with 80kg body weight) of iodinated contrast, and a slow injection rate may be used because there is no vascular phase acquisitions.
- For four step method, inject 80 ml (for a patient with 80kg body weight) of iodinated contrast media at a rate of 3-4.5ml/s.
- Inject 50-60ml of saline flush following the contrast injection.
Explanation: flushes remaining contrast in the veins of the injected hand, and maintains contrast flow for a longer time.
Important: experienced radiographer must involve when administering IV contrast because injection rate, contrast volume, and technique might be changed according to the patient body weight, patient condition, scan capturing range, and CT scanner model.
Post-processing
- Multiplanar reconstruction (MPR) images for all phases in soft-tissue window (WW:500, WL:50) with slice thickness ≤ 5mm – refer to non-contrast abdomen scan for images.
- Layered 3D images to show stones with respect to the lumbar spine.
- Curved MPR images of pre-contrast and excretory phases to show both ureters.
- 3D, MIP, curved MPR images from excretory phase to show ureters.
- Measurements of length and width of each calculus.
- Measurements of Hounsfield unit (HU) of each calculus.
Please refer non-contrast KUB and renal angiogram articles for images.
Reference
- Cellina, M., Cè, M., Rossini, N., Cacioppa, L. M., Ascenti, V., Carrafiello, G., & Floridi, C. (2023). Computed Tomography Urography: State of the Art and Beyond.Tomography (Ann Arbor, Mich.), 9(3), 909–930. https://doi.org/10.3390/tomography9030075
- O'Connor OJ, Maher MM. CT urography. AJR Am J Roentgenol. 2010 Nov;195(5):W320-4. doi: 10.2214/AJR.10.4198. PMID: 20966295.
- Olga R. Brook, MD, Chair, Jessica Kurian MD, Alec Megibow, MD, MPH, FACR, & Michael Furman, MD. (2021). ACR–SABI–SAR–SPR practice parameter for the performance of computed tomography (CT) of the abdomen and computed tomography (CT) of the pelvis.Retrieved from www.gravitas.acr.org.
- Fielding JR, Silverman SG, Rubin GD. Helical CT of the urinary tract. AJR Am J Roentgenol. 1999 May;172(5):1199-206. doi: 10.2214/ajr.172.5.10227489. PMID: 10227489.
- Coll DM, Varanelli MJ, Smith RC. Relationship of spontaneous passage of ureteral calculi to stone size and location as revealed by unenhanced helical CT. AJR Am J Roentgenol. 2002 Jan;178(1):101-3. doi: 10.2214/ajr.178.1.1780101. PMID: 11756098.
- Romanyukha, A., Nzitunga, P. S., & Dolcet, A. (2022, April 28). CT patient positioning plays key role in radiation dose reduction.www.auntminnie.com.