NCCT KUB (kidneys, ureters, bladder)
Last updated June 03, 2026
By Radiohelp Staff
Similar expressions
NCCT KUB/ CT KUB
Introduction
NCCT KUB is used to detect renal stones and locate their path in the urinary track. After recognizing renal calculi, size is accurately measured to predict the stone movement through the ureter.
Patient preparation
- Explain the procedure clearly and kindly.
- Check the suitability to expose radiation.
- Ask the patient to remove metals related to the interested region.
- Provide 1000ml of water to drink within 20-30min without emptying the urinary bladder.
Explanation: this is to adequately fill the bladder with urine, which promotes visualization of ureters.
- Start the scan when the patient’s having a fully filled bladder.
Patient positioning
- Position the patient in feet first and supine.
- Place both hands above the head.
Explanation: this reduces streak artifacts form the hands, also it avoids unnecessary radiation exposure.
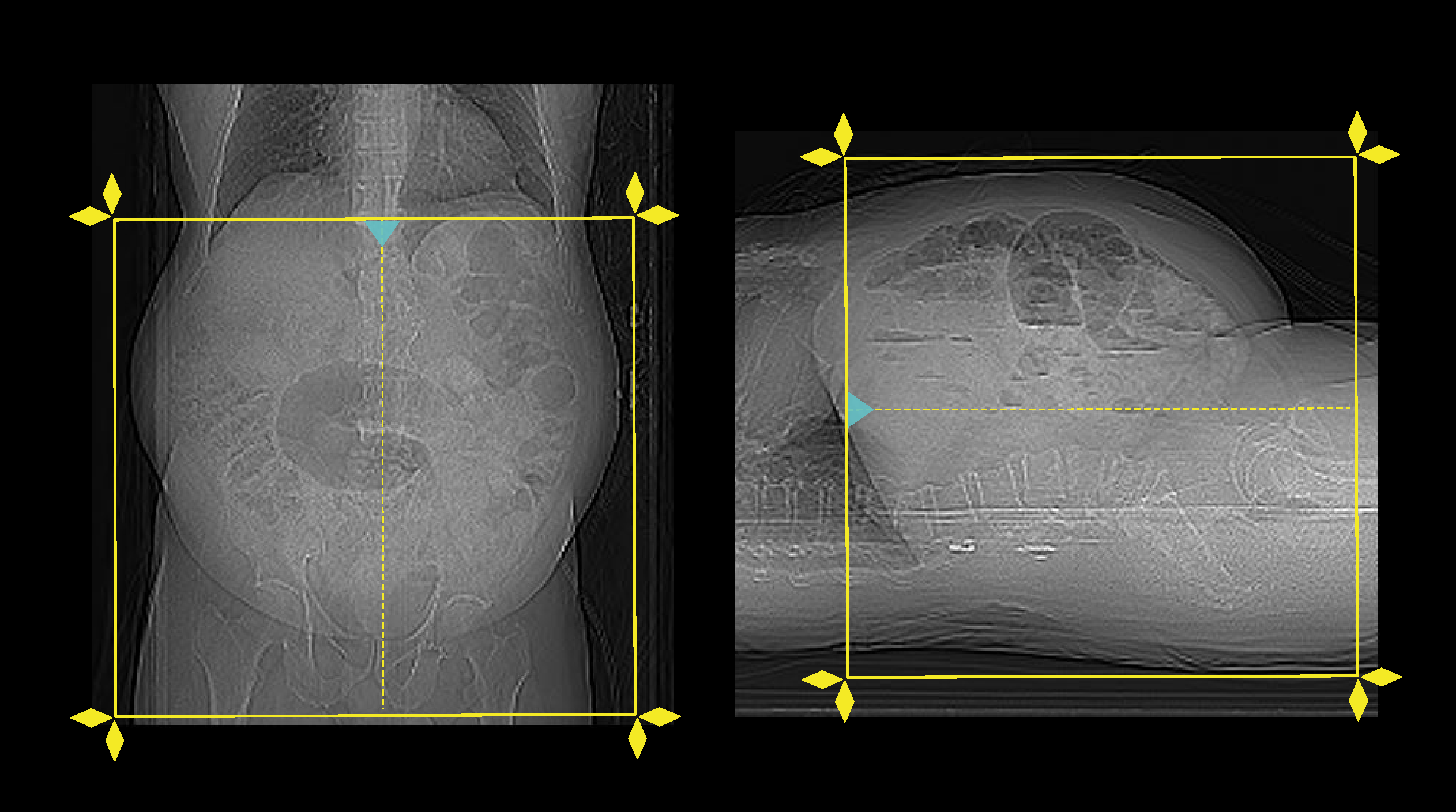
- Center the scanning area in the scanner iso-center [6].
Explanation: this reduces overall radiation exposure and increases image quality.
- Instruct the patient to breath in and hold during the scan.
Explanation: avoids motion un-sharpness of kidneys.
- Set the scout start point at the nipple level and scan direction out of the gantry.
Scan planning
Scan needs to be conducted when the patient is having a full bladder. It is usually considered that an adequately hydrated patient is having a full-bladder nearly after 45 minutes from the last urination.
- Plan the scan slab to start above kidneys and to end below pubic symphysis.
- Conduct the scan under arrested inspiration.
Post-processing
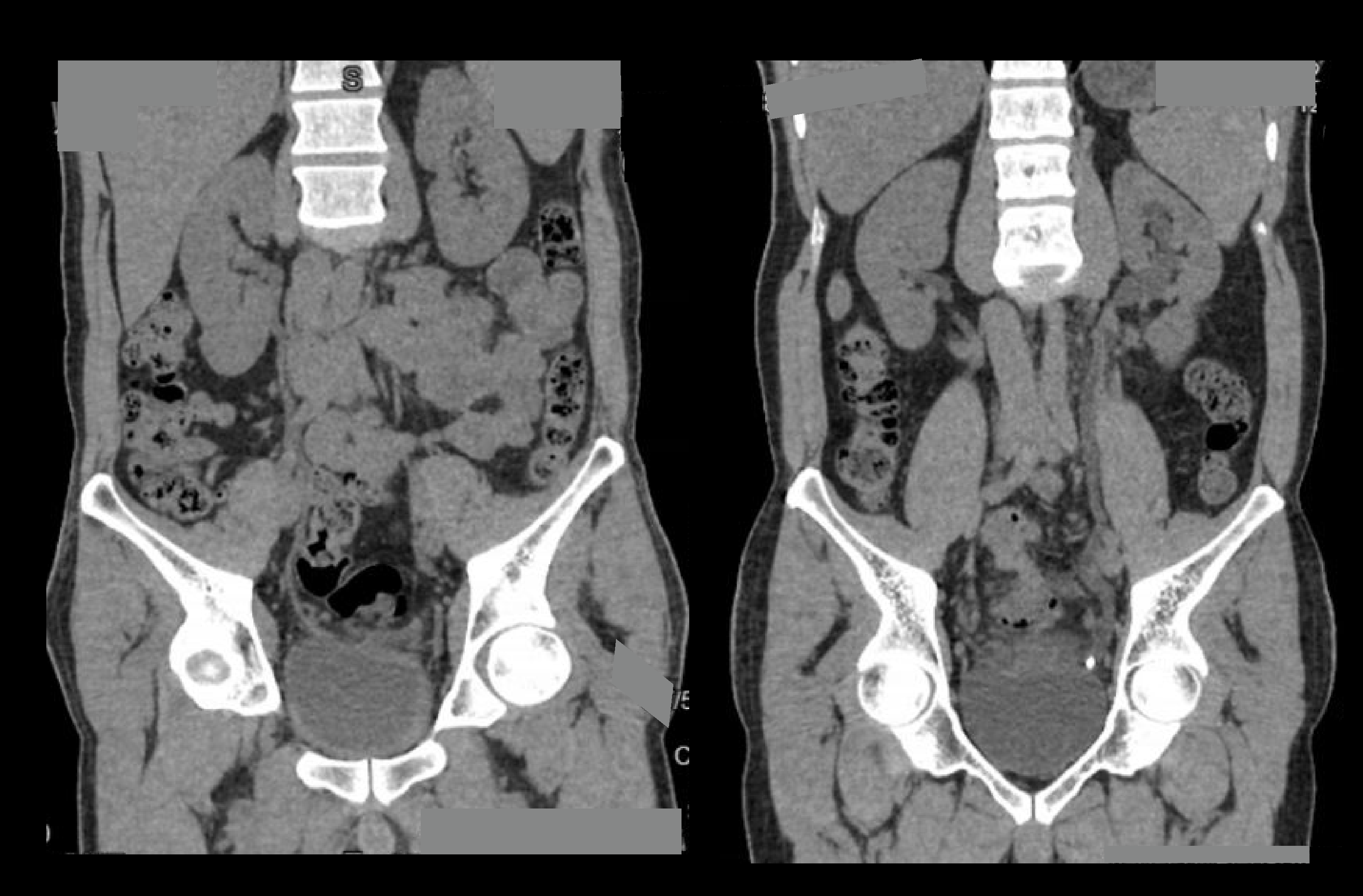
- Multiplanar reconstruction (MPR) images for all phases in soft-tissue window (WW:500, WL:50) with slice thickness ≤ 5mm – refer to non-contrast abdomen scan for images.
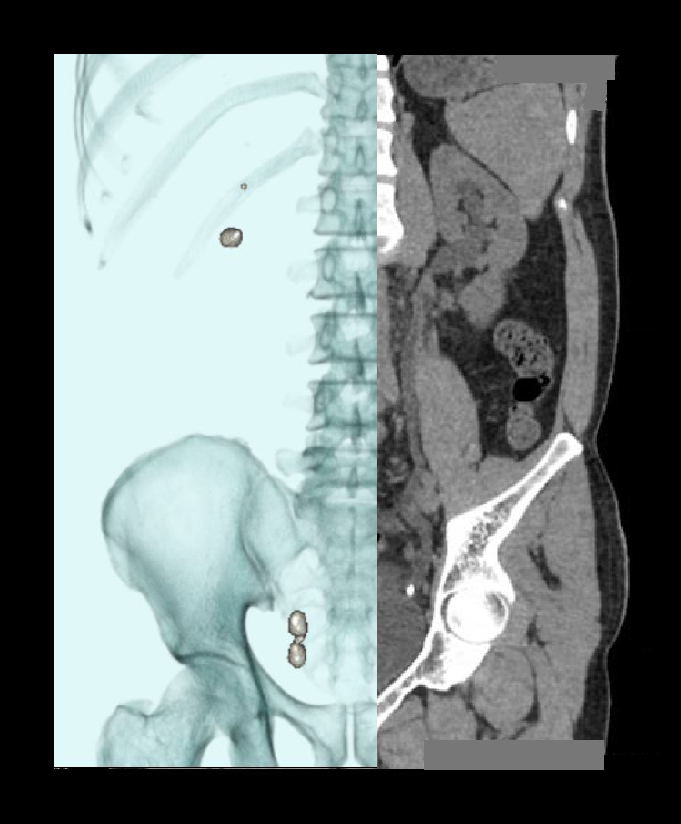
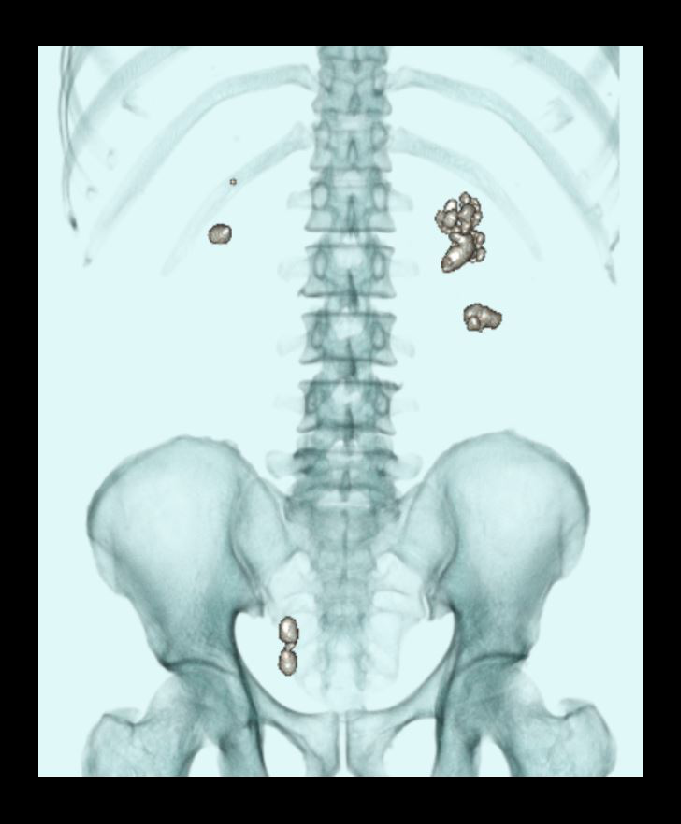
- Layered 3D images to show stones with respect to the lumbar spine.
- Curved MPR images to show both ureters.
- Measurements in length and width of each calculus.
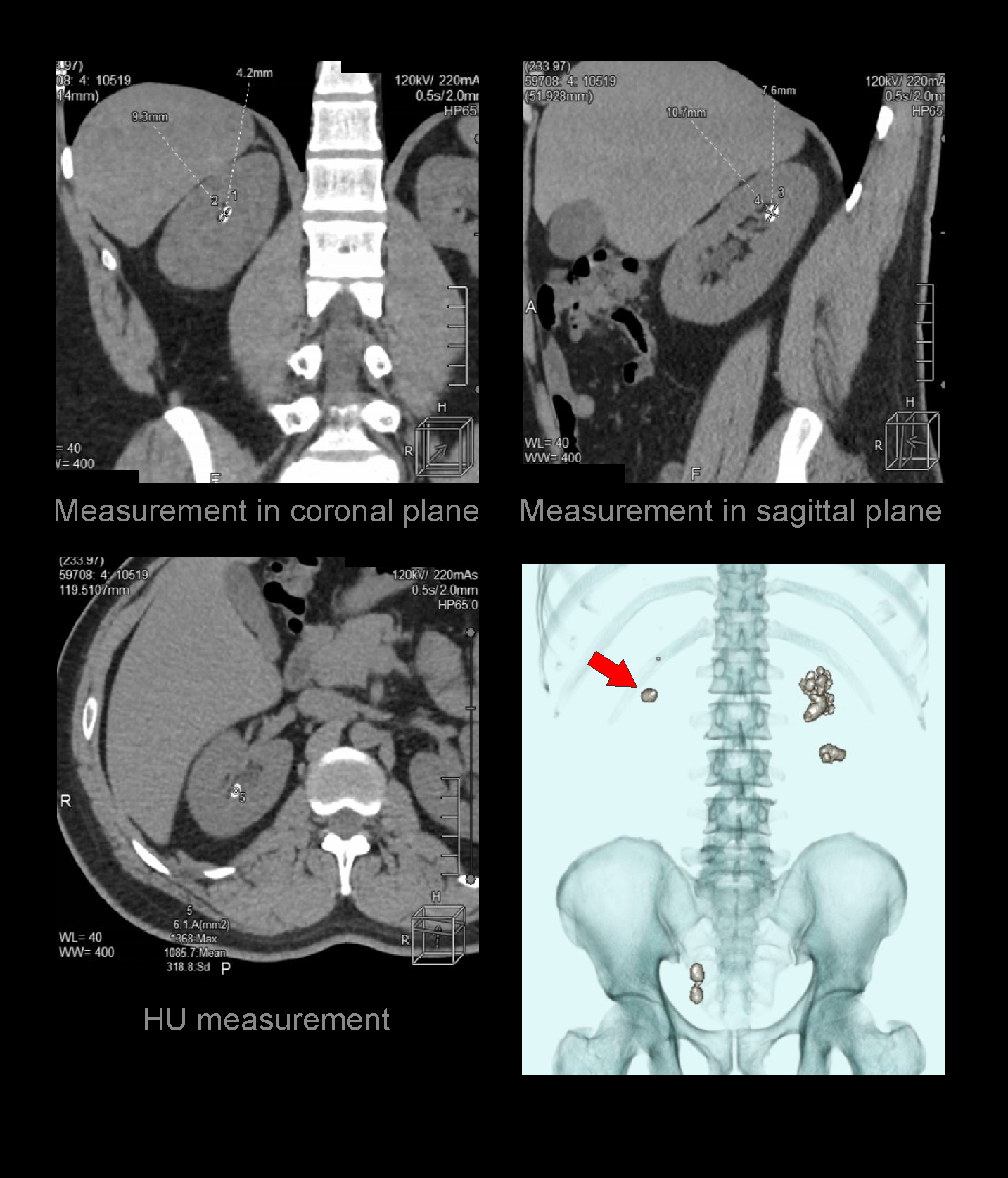
- Measurement in Hounsfield unit (HU) of each calculus.
Reference
- Patatas, K., Panditaratne, N., Wah, T. M., Weston, M. J., & Irving, H. C. (2012). Emergency department imaging protocol for suspected acute renal colic: re-evaluating our service.The British journal of radiology, 85(1016), 1118–1122. https://doi.org/10.1259/bjr/62994625
- Jarral, F., Hamdy, A., Mohamed, G., Mobayen, R., Dave, N., Eltawil, M., Mohan, A., Abusand, O.,Tokidis, E., & Akbar, J. (2024). Standardized CT KUB Protocols for Nephrolithiasis: A Retrospective Analysis of Radiation Exposure and Cranial Extent Guidelines.Cureus, 16(12), e75743. https://doi.org/10.7759/cureus.75743
- Poletti PA, Platon A, Rutschmann OT, Schmidlin FR, Iselin CE, Becker CD. Low-dose versus standard-dose CT protocol in patients with clinically suspected renal colic. AJR Am J Roentgenol. 2007 Apr;188(4):927-33. doi: 10.2214/AJR.06.0793. PMID: 17377025.
- Patti L, Leslie SW. Acute Renal Colic. [Updated 2024 Dec 23]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK431091/
- Ghoshal N, Gaikstas G. CT KUB scans for renal colic: Optimisation of scan range to reduce patient radiation burden.Radiography (Lond). 2021 Aug;27(3):784-788. doi: 10.1016/j.radi.2020.12.006. Epub 2021 Jan 13. PMID: 33451884.
- Romanyukha, A., Nzitunga, P. S., & Dolcet, A. (2022, April 28). CT patient positioning plays key role in radiation dose reduction.www.auntminnie.com.
- Olga R. Brook, MD, Chair, Jessica Kurian MD, Alec Megibow, MD, MPH, FACR, & Michael Furman,MD. (2021). ACR–SABI–SAR–SPR practice parameter for the performance of computed tomography (CT) of the abdomen and computed tomography (CT) of the pelvis.Retrieved from www.gravitas.acr.org.