CT Mesenteric angiogram
Last updated June 03, 2026
By Radiohelp Staff

Similar expressions
CT mesenteric angiogram/ CT mesenteric angiography/ CECT mesenteric angiogram/ CT mesenteric angio
Introduction
CT mesenteric angiogram helps to diagnose complications associated with the splanchnic blood circulation: aneurysm, bowel ischemia, thrombosis and stenosis. Iodinated contrast media is used to opacify the arteries, veins and bowel wall. This scan is quick and accurate for the diagnosis of acute mesenteric ischemia (AMI).
Patient preparation
- Explain the procedure clearly and kindly.
- Check contraindications for contrast media administration and radiation exposure.
- Remove metals related to the interested region.
- Place an Intra venous (IV) cannula in a stable vein of an arm – green-18G cannula.
Explanation: green cannula has higher lumen diameter, which can withstand higher flow rate.
- Prior to scan, provide 800-1000ml of negative oral contrast media such as water to drink within 30-45 minutes – this is for an adult with a body weight of 65-80kg. Administer the same amount and type of contrast media rectally.
Explanation: this is to distend bowels, improving visualization of bowel wall enhancement. Positive contrast media is not used because it suppresses bowel wall enhancement – refer multiphase contrast abdomen scan to know more details about intraluminal contrast.
- Explain and practice breath in and hold technique.
Explanation: avoids motion un-sharpness of organs and blood vessels.
Patient positioning
- Position the patient in supine and feet first on the imaging couch.
- Center the scanning area in the scanner iso-center [6].
Explanation: this reduces overall radiation exposure and increases image quality.
- Raise both hands above the head and place a positioning aide under hands.
Explanation: hands beside the trunk give streak artifacts and increase radiation exposure.
- Keep the arm with the IV cannula strait.
Explanation: to facilitate contrast flow.
- Plan the scout starting point at the nipple level.
Scan planning
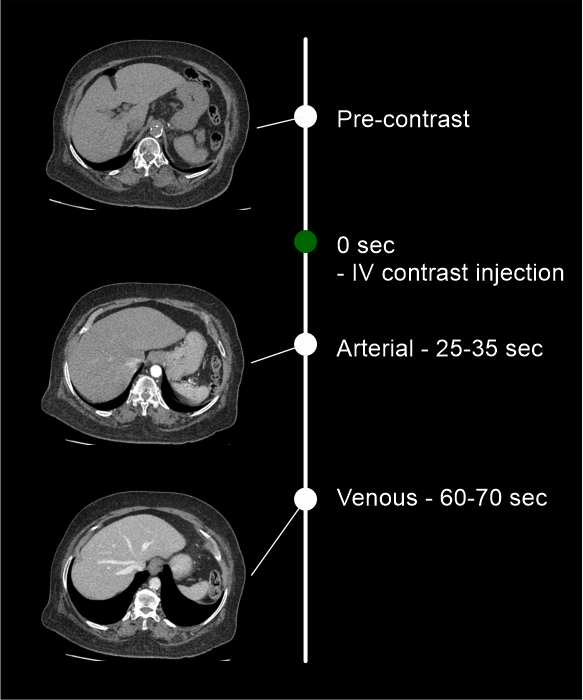
Usually, there are three steps in the scan: pre-contrast, arterial and venous. Extra delayed phasecan be added to the scan but it depends with the pathology of the patient.
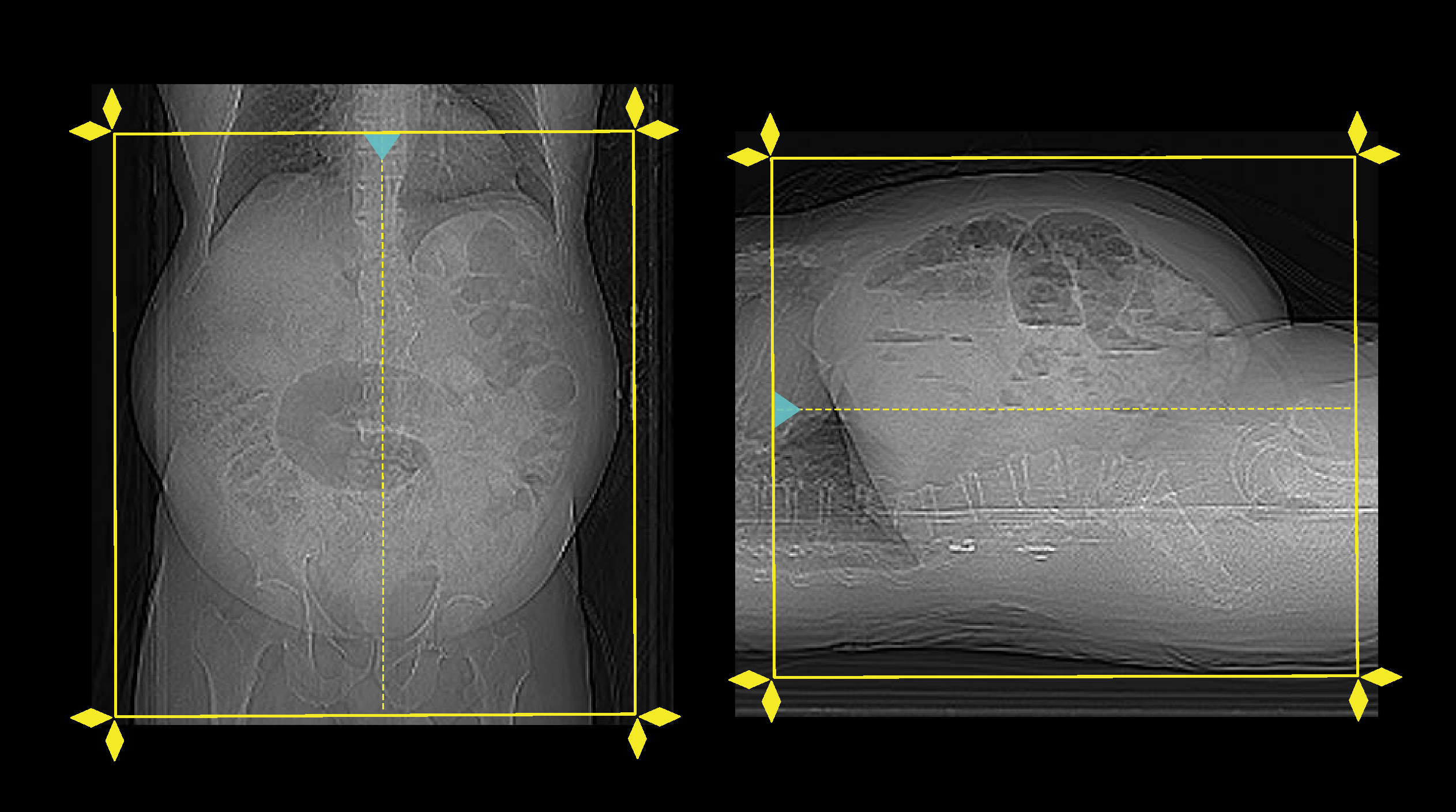
- Plan all three steps to cover from dome of the diaphragm to pubis symphysis.
- Set the phase initiation.
Explanation: Use bolus tracking method to start the angiographic phase on time. Keep a ten seconds gap between contrast initiation point and triggering point, and should not place a delay time to start the angiographic phase once the threshold value (180HU) is reached. Place scan-and-view slice (S and V) just above the diaphragm. Please refer abdominal aortogram scan for images.
Intravenous (IV) contrast infusion
- Inject 80 ml (for a patient with 70-80kg body weight) of iodinated contrast media at a rate of 4.5-5ml/s.
- Inject 50-60ml of saline flush following the contrast injection.
Explanation: flushes remaining contrast in the veins of the injected hand, and maintains contrast flow for a longer time.
- Conduct all phases under arrested inspiration.
Important: when administering IV contrast, factors such as injection rate, volume, and technique might be changed according to the patient body weight, patient condition, scan capturing range, and CT scanner model.
Post-processing
- Multiplanar reconstruction (MPR) images for all phases in soft-tissue window (WW:500, WL:50) with slice thickness ≤ 5mm – refer to non-contrast abdomen scan for images.
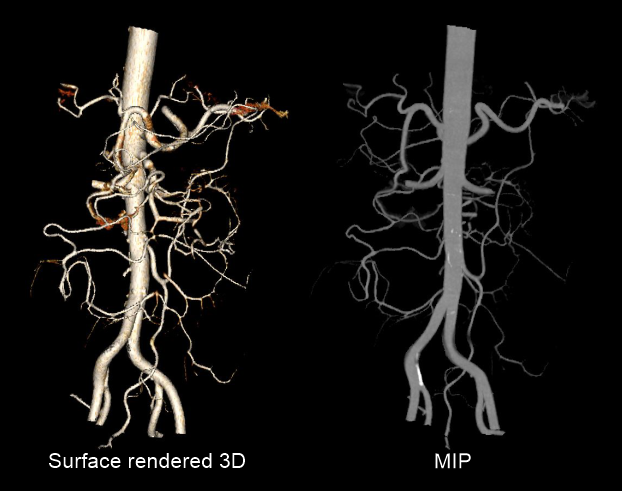
- Surface rendered 3D and Maximum intensity projection (MIP) images of mesenteric arteries.
- Axial images in bone window (WW: 3500, WL: 350) with ≤ 3mm slice thickness.
Reference
- Steven S. Raman, MD, Chair, Dorothy Gilbertson, MD, & Charles White, MD. (2021). ACR–NASCI–SIR–SPR Practice parameter for the performance and interpretation of body computed tomography angiography (CTA). Retrieved from www.gravitas.acr.org.
- Kirkpatrick ID, Kroeker MA, Greenberg HM. Biphasic CT with mesenteric CT angiography in the evaluation of acute mesenteric ischemia: initial experience. Radiology. 2003 Oct;229(1):91-8. doi: 10.1148/radiol.2291020991. Epub 2003 Aug 27. PMID: 12944600.
- Garzelli L, Nuzzo A, Copin P, Calame P, Corcos O, Vilgrain V, Ronot M. Contrast-Enhanced CT for the Diagnosis of Acute Mesenteric Ischemia.AJR Am J Roentgenol. 2020 Jul;215(1):29-38. doi: 10.2214/AJR.19.22625. Epub 2020 May 6. PMID: 32374661.
- Guglielmo FF, Wells ML, Bruining DH, Strate LL, Huete Á, Gupta A, Soto JA, Allen BC, Anderson MA, Brook OR, Gee MS, Grand DJ, Gunn ML, Khandelwal A, Park SH, Ramalingam V, Sokhandon F, Yoo DC, Fidler JL. Gastrointestinal Bleeding at CT Angiography and CT Enterography: Imaging Atlas and Glossary of Terms.Radiographics. 2021 Oct;41(6):1632-1656. doi: 10.1148/rg.2021210043. PMID: 34597220.
- Di Serafino, M., Iacobellis, F., Schillirò, M. L., Dell'Aversano Orabona, G., Martino, A., Bennato, R., Borzelli, A., Oliva, G., D'Errico, C., Pezzullo, F., Barbuto, L., Ronza, R., Ponticiello, G., Corvino, F., Giurazza, F., Lombardi, G., Niola, R., & Romano, L. (2022). The Role of CT-Angiography in the Acute Gastrointestinal Bleeding: A Pictorial Essay of Active and Obscure Findings.Tomography (Ann Arbor, Mich.), 8(5), 2369–2402. https://doi.org/10.3390/tomography8050198
- Romanyukha, A., Nzitunga, P. S., & Dolcet, A. (2022, April 28). CT patient positioning plays key role in radiation dose reduction.www.auntminnie.com.