CT Pulmonary angiogram (CTPA)
Last updated April 29, 2026
Similar expressions
CTPA, CT pulmonary angio, CT pulmonary angiography, CT pulmonary angio contrast, CTPE
Introduction
CTPA is a special study that is used to diagnose pulmonary embolisms. Contrast media is used to enhance the main pulmonary artery and its branches.
Patient preparation
- Explain the procedure clearly and kindly.
- Remove metals related to the scanning area (underwear, necklaces).
- Check contraindications for contrast media administration and radiation exposure.
- Place an Intra venous (IV) cannula in a stable vein of the right arm – green-18G cannula.
Explanation: Green cannula has higher lumen diameter, which can withstand higher flow rate. A right arm injection is preferred in thoracic CTA because to avoid streak artifacts from undiluted contrast media in the left brachiocephalic vein.
- Practice breathing technique, breath in and hold at a comfortable level without having a fullinspiration.
Explanation: holding the breadth at a full inspiration can reduce blood flow through the pulmonary trunk, resulting minimally enhanced pulmonary arteries.
Patient positioning
- Position the patient in supine and feet first on the imaging couch.
- Center the scanning area in the scanner iso-center [6].
Explanation: this reduces overall radiation exposure and increases image quality.
- Raise both hands above the head and place a positioning aide under them.
Explanation: hands beside the trunk give streak artifacts and increase radiation exposure.
- Keep strait the arm with the IV cannula.
Explanation: to facilitate contrast flow.
- Plan scan starting point at the lower neck.
Scan planning
Usually, only arterial phase is performed, but pre-contrast step can be included according to diagnostic needs of the patient.
- Plan the scan slab to cover from lung apex to posterior costophrenic sulci.
Arterial phase initiation is comparatively a challenge in CTPA because contrast reach pulmonary trunk before it reaches lungs and aorta. It is important to remember that late acquisition causes pulmonary veins to appear in images, which makes it hard to differentiate pulmonary arteries from veins. Therefore, scan acquisition should be quick and on-time, and this can be achieved by either test bolus or bolus tracking method.
Method 1 - bolus tracking
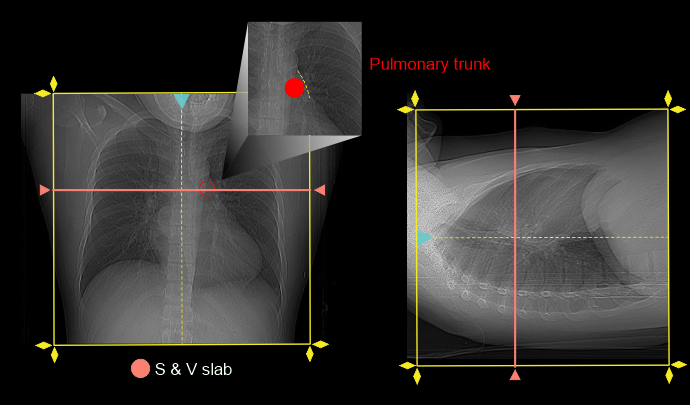
- Place scan and view (S & V) slab at the mid-level of pulmonary trunk.
- No delay time between arterial scan and S & V.
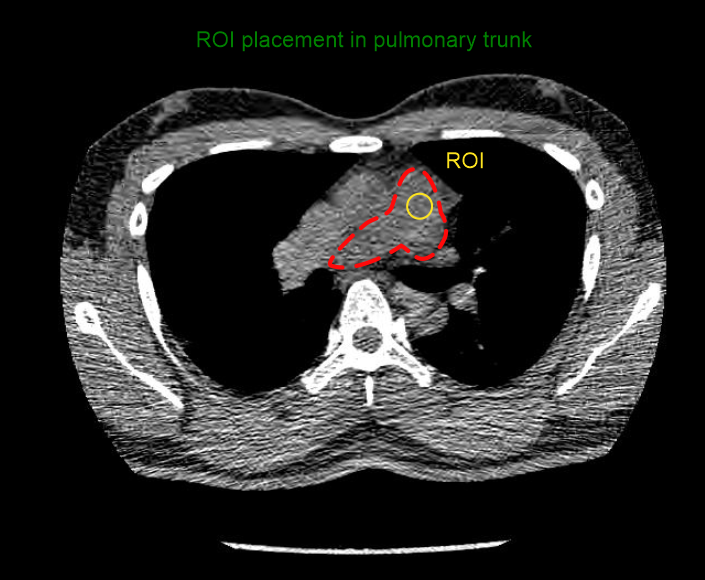
- Place triggering ROI in the pulmonary trunk.
- Preset breadth hold command to start after 6 seconds from contrast injection.
Explanation: this is to avoid a delayed acquisition. In detail, it takes nearly 5 seconds to complete a breadth hold command, and that time is just right to delay the scan. However, an early breadth hold is achieved by making the patient to hold the breadth prior to pulmonary enhancement.
- Preset threshold value to 180 Hounsfield units (HU).
You can find a detailed explanation of bolus-tracking technique in our thoracic aortogram article.
Method 2 - test-bolus
- Follow S & V slice and triggering ROI placement as mentioned in the bolus tracking method.
- Use 10ml of contrast media with the same injection rate (4.5-5 ml/s) for the CTP scan.
- Start triggering and contrast injection simultaneously.
- Record equipment delay plus breadth hold time (Y).
- Record the time it takes to reach 180 HU in the time density curve (X).
- Use X minus Y as the preset time for the scan to start.
Intravenous (IV) contrast infusion
- Inject 60-65 mL (65kg body weight, 640 slice scanner) of iodinated contrast at a rate of 4.5-5mL/s.
- Inject 50-60 mL of saline flush following contrast injection - with the same injection rate.
Explanation: helps to flush remaining contrast in veins and maintains a longer contrast flow time.
Final enhancement of pulmonary arteries should be above 250-300 HU to detect arterial pathologies.
Post-processing
- Axial, coronal and sagittal images with ≤3-5mm slice thickness in soft-tissue window.
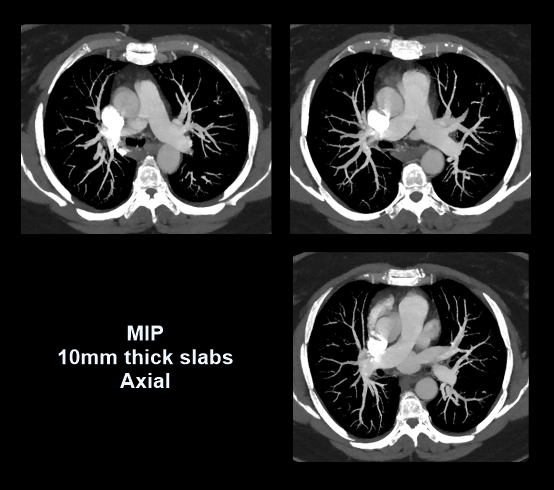
- Overlapping maximum intensity projection (MIP) images with 5-10mm slab thickness, in transverse plane.
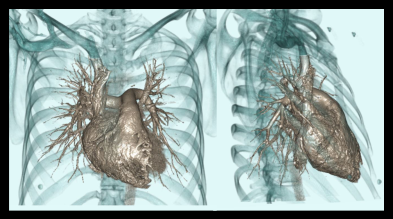
- 3D surface shaded images and MIP images.
- Curved planner reformation (CPR) images of affected arteries.
- Axial images with <3 mm slice thickness in both lung (WW: 1500, WL: -500) and bone window (WW: 3500, WL: 350).
Please refer to our chest non-contrast article for more images on multiplanar reformation (MPR).
Reference
- Ravula, P., Mohanakrishnan, A., Muralidharan, Y., Kanadasan, K., & Natarajan, P.(2024). The Role of Advanced Post-processing Techniques in Computed Tomography Pulmonary Angiography for the Accurate Diagnosis of Pulmonary Thromboembolism: A Retrospective Study.Cureus, 16(8), e67583. https://doi.org/10.7759/cureus.67583
- Aldosari S, Jansen S, Sun Z. Optimization of computed tomography pulmonary angiography protocols using 3D printed model with simulation of pulmonary embolism.Quant Imaging Med Surg. 2019 Jan;9(1):53-62. doi: 10.21037/qims.2018.09.15. PMID: 30788246; PMCID: PMC6351811.
- Grob D, Oostveen LJ, Prokop M, Schaefer-Prokop CM, Sechopoulos I, Brink M. Imaging of pulmonary perfusion using subtraction CT angiography is feasible in clinical practice.Eur Radiol. 2019 Mar;29(3):1408-1414. doi: 10.1007/s00330-018-5740-4. Epub 2018 Sep 25. PMID: 30255247; PMCID: PMC6510874.
- Nguyen ET, Hague C, Manos D, Memauri B, Souza C, Taylor J, Dennie C. Canadian Society of Thoracic Radiology/Canadian Association of Radiologists Best Practice Guidance for Investigation of Acute Pulmonary Embolism, Part 1: Acquisition and Safety Considerations.Can Assoc Radiol J. 2022 Feb;73(1):203-213. doi: 10.1177/08465371211000737. Epub 2021 Mar 29. PMID: 33781098.
- Zhao, Y., Hubbard, L., Malkasian, S., Abbona, P., Bosemani, V., & Molloi, S. (2023). A patient-specific timing protocol for improved CT pulmonary angiography.Research in diagnostic and interventional imaging, 8, 100036. https://doi.org/10.1016/j.redii.2023.100036
- Romanyukha, A., Nzitunga, P. S., & Dolcet, A. (2022, April 28). CT patient positioning plays key role in radiation dose reduction.www.auntminnie.com.
- Wu, H., Chen, X., Zhou, H., Qin, B., Cao, J., Pan, Z., & Wang, Z. (2020). An optimized test bolus for computed tomography pulmonary angiography and its application at 80 kV with 10 mL contrast agent.Scientific reports, 10(1), 10208. https://doi.org/10.1038/s41598-020-67145-9
- Steven S. Raman, MD, Chair, Dorothy Gilbertson, MD, & Charles White, MD. (2021). ACR–NASCI–SIR–SPR Practice parameter for the performance and interpretation of body computed tomography angiography (CTA).Retrieved from www.gravitas.acr.org.
- Murphy A, White H. A comparison of bolus track and test bolus computed tomography pulmonary angiography and the implications on pulmonary and aortic vessel enhancement, effective dose and suboptimal scan rate.J Med Radiat Sci. 2024 Mar;71(1):44-50. doi: 10.1002/jmrs.724. Epub 2023 Sep 7. PMID: 37675768; PMCID: PMC10920937.
- Mannudeep K. S. Kalra, MD, Chair, Jessica Kurian MD, & Satinder Singh, MD, FSABI. (2023). ACR–SABI–SPR–STR Practice parameter for the performance of thoracic computed tomography (CT). Retrieved from www.gravitas.acr.org.