CT Neck (Non-Contrast)
Last updated January 25, 2026
Similar expressions
CT Neck/ NCCT neck/ non-contrast neck
Introduction
CT Neck scan is used for the assessment of congenital abnormalities, foreign body, neoplasms, trauma and palpable masses. In usual practice, non-contrast neck step is combined with contrast steps such as 4D neck and neck-contrast for complex diagnosis.
Patient preparation
- Explain the procedure kindly and clearly.
- Remove metal related to the neck area (necklaces, undergarments).
- Ask to be steady and not to swallow during the procedure.
- Inform to breath slowly during the procedure.
Patient positioning
- Position in head-first and supine position.
- Center the scanning area in the scanner iso-center [5].
Explanation: this reduces overall radiation exposure and increases image quality.
- Extend the neck slightly.
Explanation: reduces streak artifacts or beam hardening artifacts due to the lower jaw. Same results can be achieved by angulating CT gantry.
- Position the shoulders in a pulled down position and arms next to the body.
Explanation: reduces streak artifacts or beam hardening artifacts due to wide shoulders. Placing a cushion under mid-upper thorax moves shoulders posteriorly, and helps to reduce streak artifacts at the root of the neck [2].
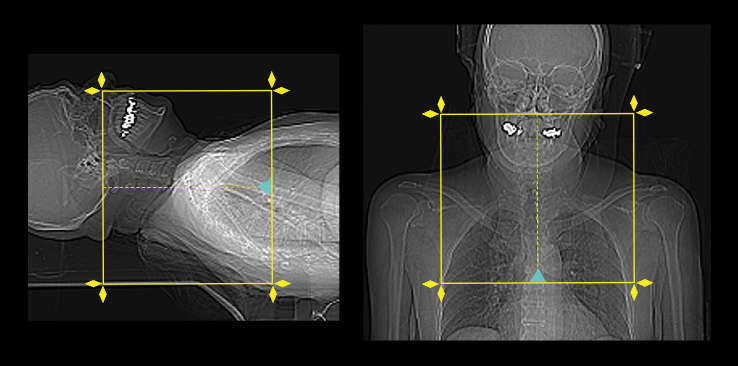
- Plan the scout starting point at the level of clavicles.
Scan planning
- Plan the scan slab to cover from the skull base to the top of the aortic-arch.
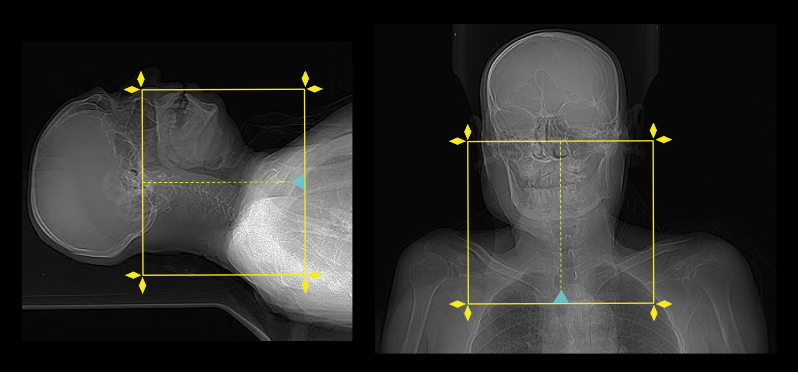
- For studies to assess vocal cord palsy, the inferior extent of the scan area should extend to aortopulmonary window or carina.
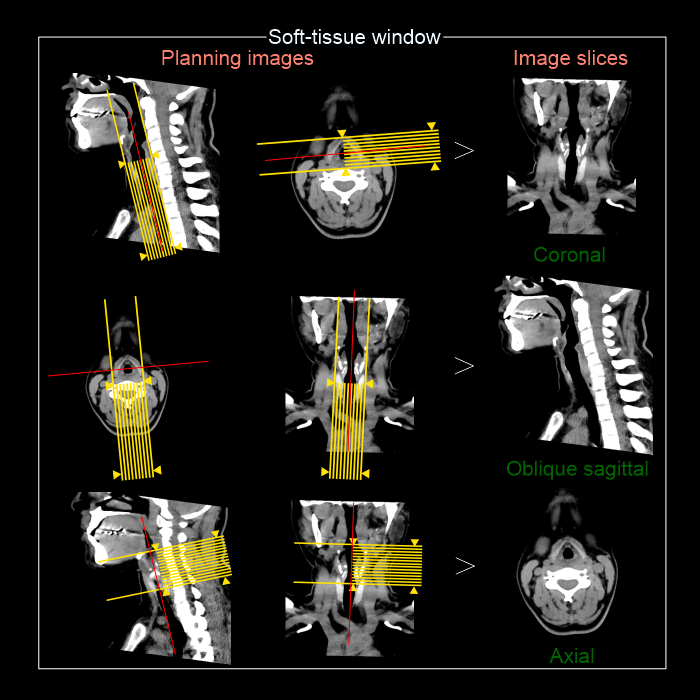
Post-processing
- Axial, coronal and sagittal images in soft-tissue window (WW: 400, WL:40), without exceeding 3mm slice thickness – reach our Neck contrast article for images.
- Additionally, a suitable image in bone (WW: 3500, WL:350) window, displayed in any plane, without exceeding 3mm slice thickness.
- For vocal cord neoplasms, 1mm thin sections of multi planer reformats (MPR) are helpful insoft-tissue window limited to the larynx, and axial slices are reformatted parrel to the vocal cords or hyoid bone.
Reference
- Ashley H. Aiken, MD, Chair, Paul M. Bunch, MD, & Kavita K. Erickson, MD. (2021). ACR–ASNR–SPR Practice parameter for the performance of computed tomography (CT) of the extracranial head and neck.Retrieved from www.gravitas.acr.org.
- Harvey, G. D., Mayer, D. P., & Radecki, P. D. (1984). Simplified patient positioning to reduce beam hardening in CT of the lower neck. AJNR. American journal of neuroradiology, 5(6), 796.
- Chin SC, Edelstein S, Chen CY, Som PM. Using CT to localize side and level of vocal cord paralysis.AJR Am J Roentgenol. 2003 Apr;180(4):1165-70. doi: 10.2214/ajr.180.4.1801165. PMID: 12646476.
- Becker M, Leuchter I, Platon A, Becker CD, Dulguerov P, Varoquaux A. Imaging of laryngeal trauma.Eur J Radiol. 2014 Jan;83(1):142-54. doi: 10.1016/j.ejrad.2013.10.021. Epub 2013 Oct 27. PMID: 24238937.
- Romanyukha, A., Nzitunga, P. S., & Dolcet, A. (2022, April 28). CT patient positioning plays key role in radiation dose reduction.www.auntminnie.com.
- Bashir MH, Joyce C, Bolduan A, Sehgal V, Smith M, Charous SJ. Revisiting CT Signs of Unilateral Vocal Fold Paralysis: A Single, Blinded Study. AJNR Am J Neuroradiol. 2022 Apr;43(4):592-596. doi: 10.3174/ajnr.A7451. Epub 2022 Mar 24. PMID: 35332018; PMCID: PMC8993190.