CT Wrist Joint scan
Last updated June 03, 2026
By Radiohelp Staff

Similar expressions
CT wrist joint/ NCCT wrist
Introduction
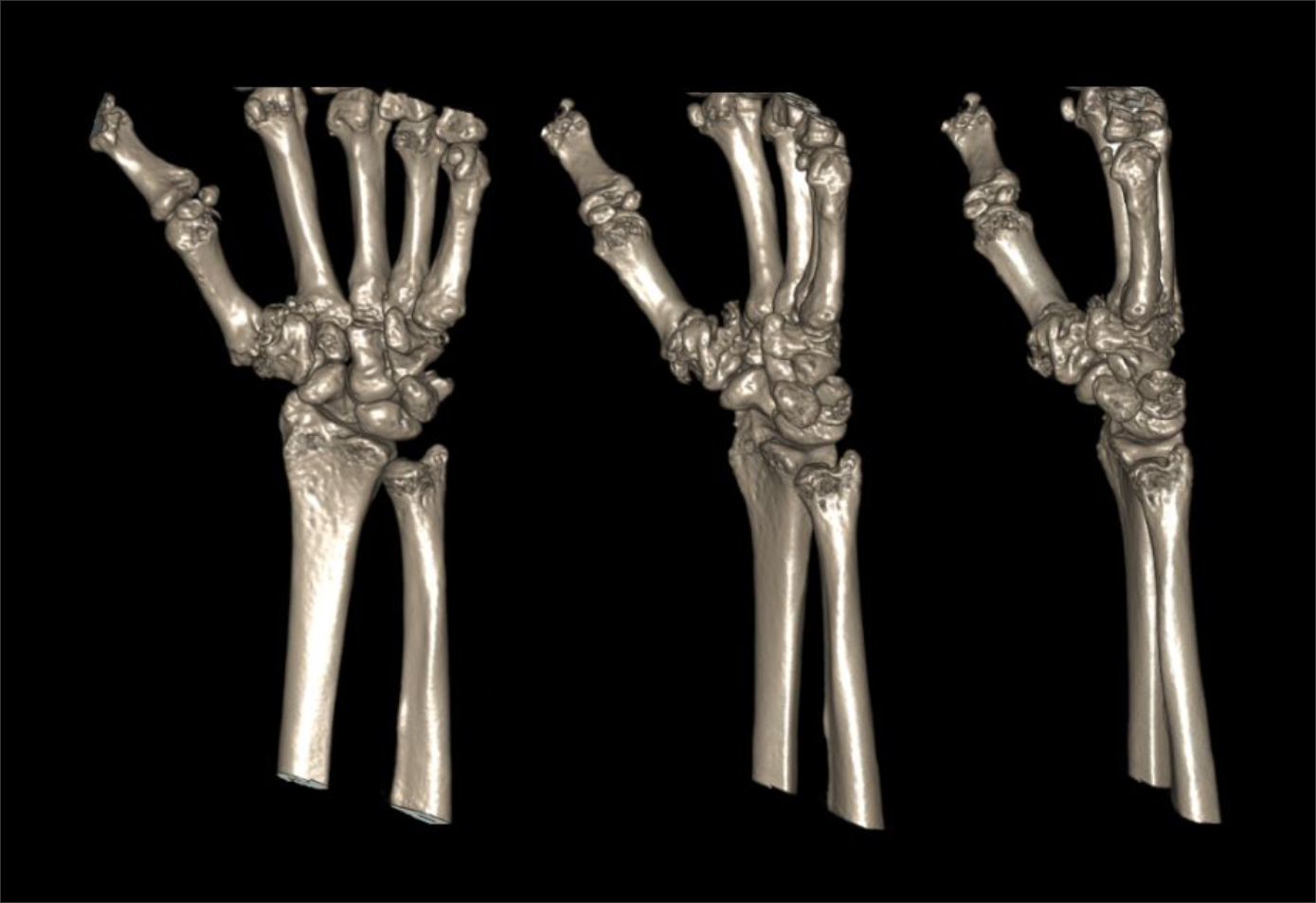
CT wrist joint scan is used to evaluate fractures, implant complications and neoplasm. Its ability to view structures in three dimension (3D) is remarkable for surgical planning.
Patient preparation
- Explain the procedure kindly and clearly.
- Remove radio opaque items related to the interested region.
Patient positioning
There are several positioning methods for CT wrist scan.
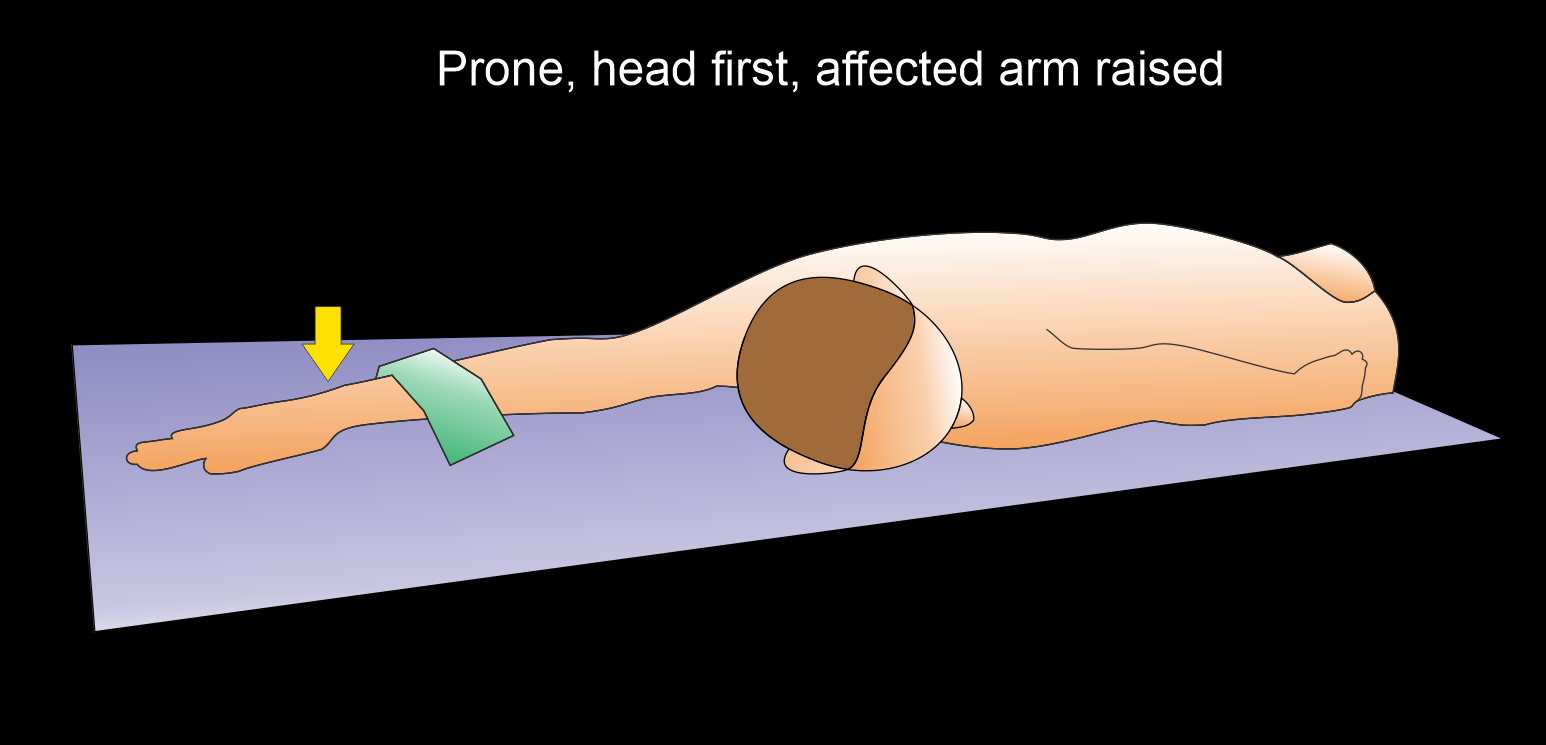
Method 1 - patient in prone, head first.
- Raise the affected arm above the head and keep the unaffected arm besides the body.
- Center the affected wrist in the iso-center.
Explanation: hand in the iso-center helps to reduce radiation exposure and increases image quality.
- Pronate the hand.
- Bend patient’s head towards unaffected arm.
- Place a sand bag on the proximal one third of the affected forearm to immobilize.
- Ask not to move the hand.
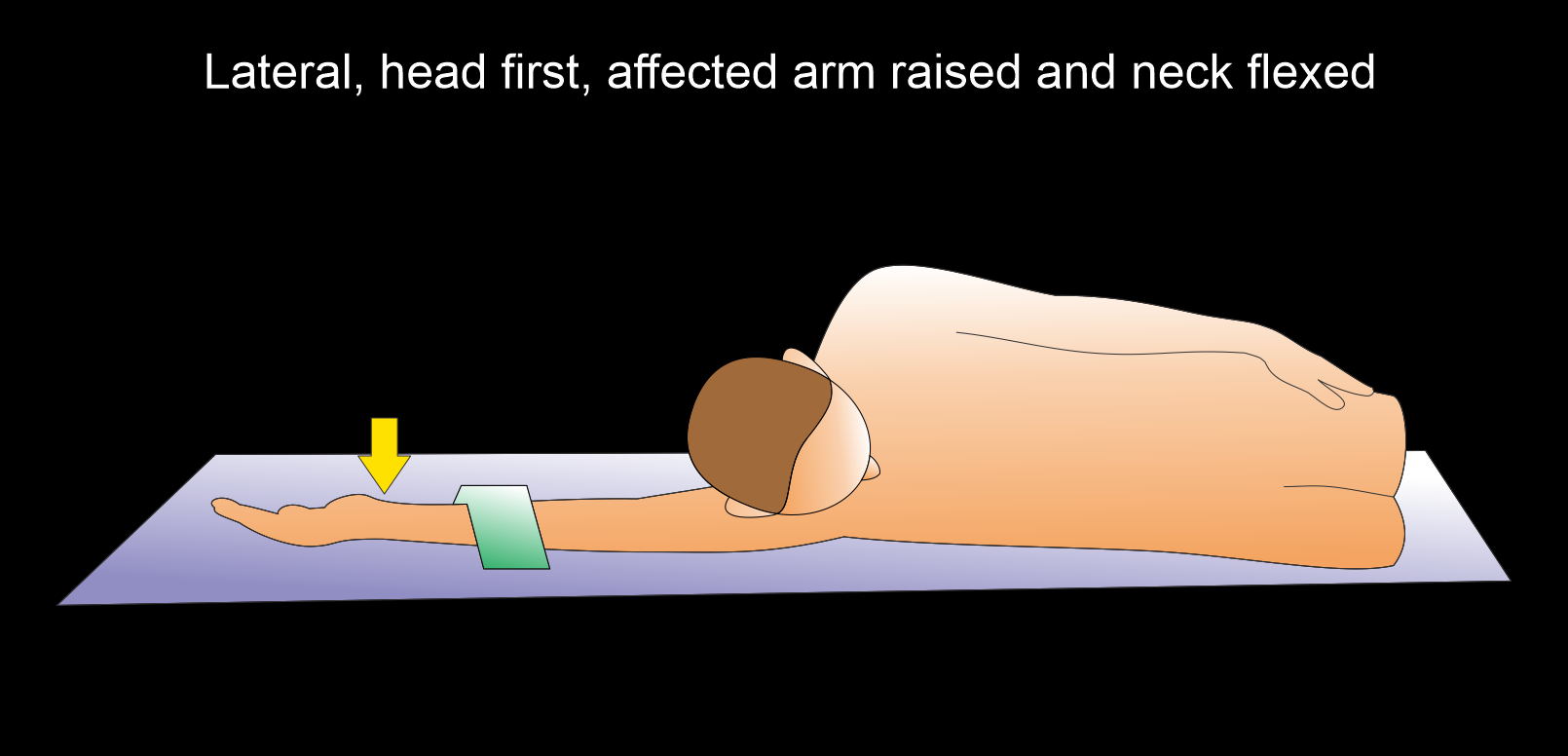
Method 2 - patient in lateral decubitus, head first.
- Position the patient in lateral decubitus on the affected side.
- Raise the affected arm above the head.
- Supinate the hand.
- Place a sand bag on the proximal one third of the affected forearm to immobilize.
- Ask not to move the hand.
Explanation: this method is suitable for the patients who are unable to be in prone position.
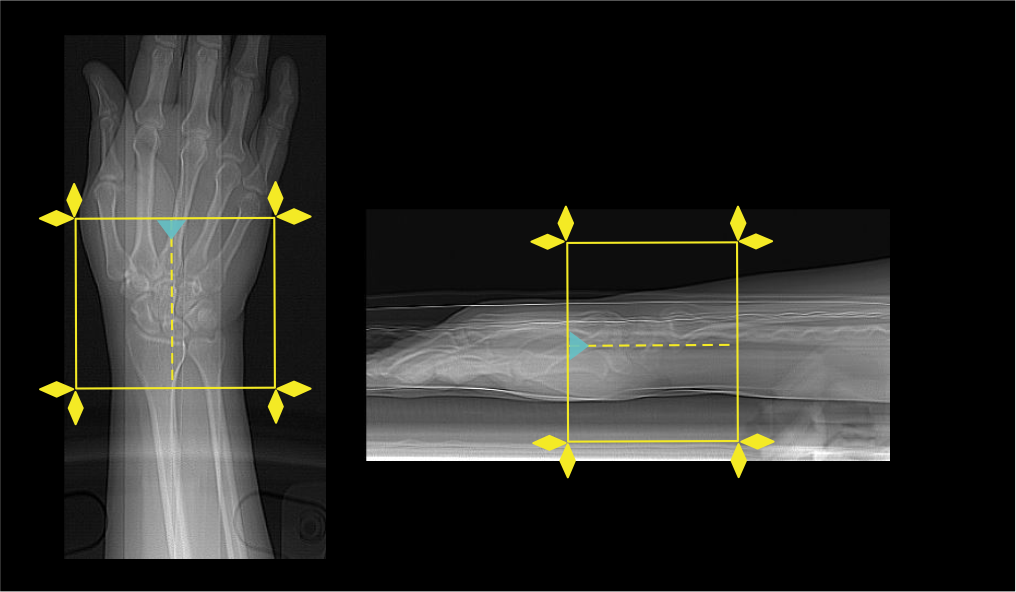
Scan planning
- Plan the scan slab to cover from the radioulnar joint to base of the metacarpals.
- Reduce the field of view (FOV) as appropriate to include wrist joint.
Explanation: small FOV increases geometric resolution.
Post-processing
- Coronal, sagittal and axial images in both soft tissue (WW:500, WL:50) and bone (WW: 3500, WL: 350) window with ≤2mm slice thickness.
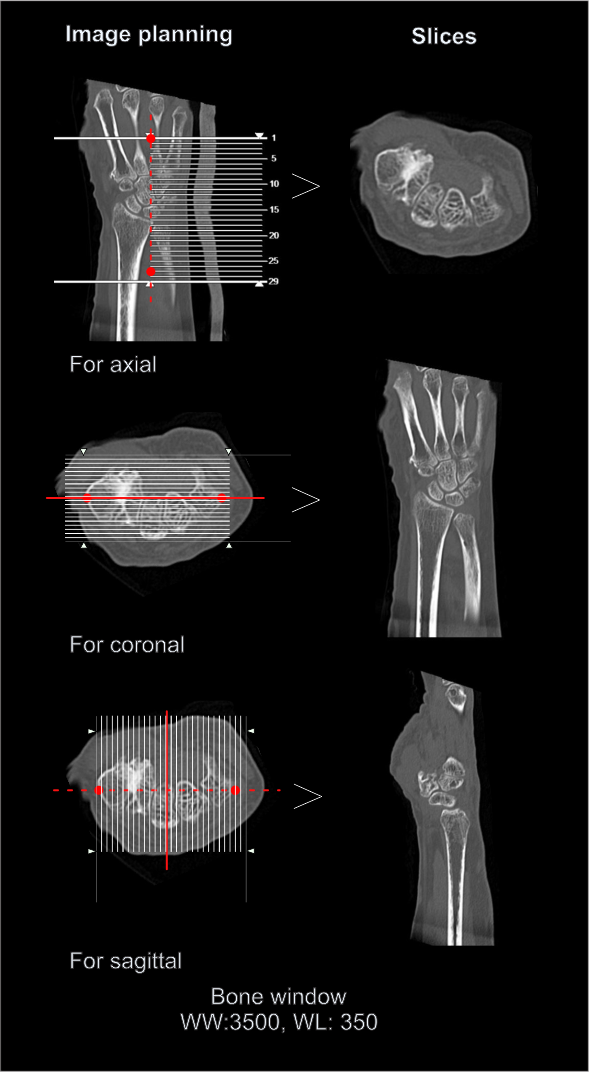
- 3d images to show pathologies clearly.
Reference
- Assi A. A. (2011). Wrist: Different views in CT scanning. Polish journal of radiology, 76(2), 40–42.
- Leng, S., Zhao, K., Qu, M., An, K. N., Berger, R., & McCollough, C. H. (2011). Dynamic CT technique for assessment of wrist joint instabilities. Medical physics, 38 Suppl 1(Suppl 1), S50. https://doi.org/10.1118/1.3577759
- van den Bergh E, Dobbe I, Streekstra GJ. 4D CT acquisition methods and their anticipated effects on image quality in dynamic CT-scanning of the wrist.Z Med Phys. 2025 Apr 17:S0939-3889(25)00036-4. doi: 10.1016/j.zemedi.2025.03.001. Epub ahead of print. PMID: 40251111.
- Kleinlugtenbelt YV, Madden K, Groen SR, Ham SJ, Kloen P, Haverlag R, Simons MP, Bhandari M, Goslings JC, Scholtes VAB, Poolman RW. Can experienced surgeons predict the additional value of a CT scan in patients with displaced intra-articular distal radius fractures?Strategies Trauma Limb Reconstr. 2017 Aug;12(2):91-97. doi: 10.1007/s11751-017-0283-9. Epub 2017 Apr 24. PMID: 28439818; PMCID: PMC5505880.
- Brink, M., Steenbakkers, A., Holla, M., de Rooy, J., Cornelisse, S., Edwards, M. J.,& Prokop, M. (2019). Single-shot CT after wrist trauma: impact on detection accuracy and treatment of fractures. Skeletal radiology, 48(6), 949–957. https://doi.org/10.1007/s00256-018-3097-z
- Romanyukha, A., Nzitunga, P. S., & Dolcet, A. (2022, April 28). CT patient positioning plays key role in radiation dose reduction.www.auntminnie.com.
- Xiao, M., Zhang, M., Lei, M., Lin, F., Chen, Y., Chen, J., Liu, J., & Ye, J. (2023). Diagnostic accuracy of ultra-low-dose CT compared to standard-dose CT for identification of non-displaced fractures of the shoulder, knee, ankle, and wrist. Insights into imaging, 14(1), 40. https://doi.org/10.1186/s13244-023-01389-7