Chest HRCT
Last updated July 01, 2026
By Radiohelp Staff
Similar expressions
HRCT chest/ High-resolution chest/ NC HRCT chest
Introduction
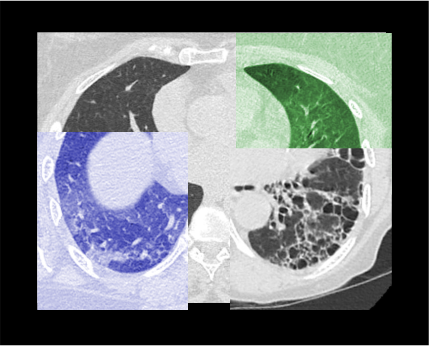
Chest HRCT is a special scan that is used to diagnose conditions related to lung parenchyma and airways, including diffuse lung disease, small airway disease, treatment evaluations and lung biopsy guidance. Images of this scan has high-resolution because they are created using high-spatial-frequency reconstruction algorithm.
Patient preparation
- Explain the procedure clearly and kindly.
- Ask the patient to remove metals related to the scanning area (underwear and necklaces).
- Practice breathing technique for the scan – routinely it’s arrested full-inspiration.
Explanation: routinely, scan is conducted under arrested full inspiration with patient in supine position. Additionally, prone or end-expiratory images may be taken for disease categorization – a detailed explanation is added to the post processing section.
Patient positioning
- Position the patient in supine and feet first on the imaging couch.
- Both hands are raised above the head and place a positioning aide or a pillow under the hands for comfort.
Explanation: this reduces streak artifacts from the hands, and also avoids unnecessary radiation exposure to the hands.
- For prone position, prone on the couch with hands raised and flexed above a pillow, and head turned laterally.
- Center the scanning area in the scanner iso-center [6].
Explanation: this reduces overall radiation exposure and increases image quality.
- Plan the scan starting point at the lower neck.
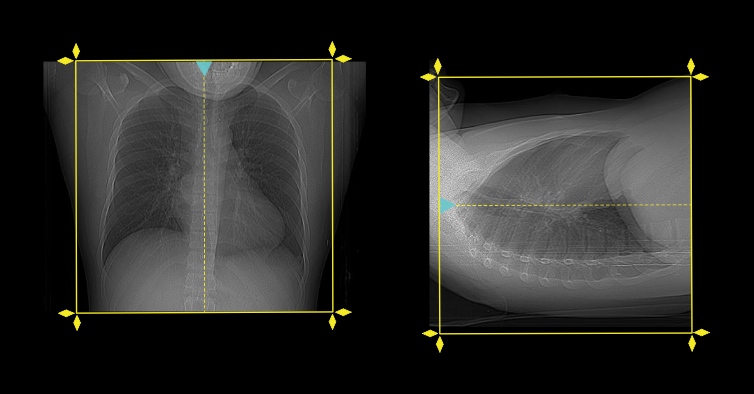
Scan planning
- Plan the scanning slab to cover from the lung apex to posterior costophrenic sulci.
- Scan is acquired in suspended full inspiration or additional steps can be added on request.
Post-processing
- Axial, coronal and sagittal images with ≤1.5 mm slice thickness in lung window (WW: 1500, WL: -500), reconstructed in high spatial frequency reconstruction algorithm.
- Field of view (FOV) of lung window should be reduced to rib cage.
Explanation: to increase spatial resolution of the image, and this is specific for diffuse lung diseases.
- Axial, coronal and sagittal images with <5mm slice thickness in soft-tissue window.
- Axial images with <3mm slice thickness in bone window (WW: 3500, WL: 350).
- FOV of soft-tissue and bone windows should include skin margins.
- Overlapping maximum intensity projection (MIP) images with 5-10mm slab thickness, intransverse plane.
Explanation: helps to detect lung nodules.
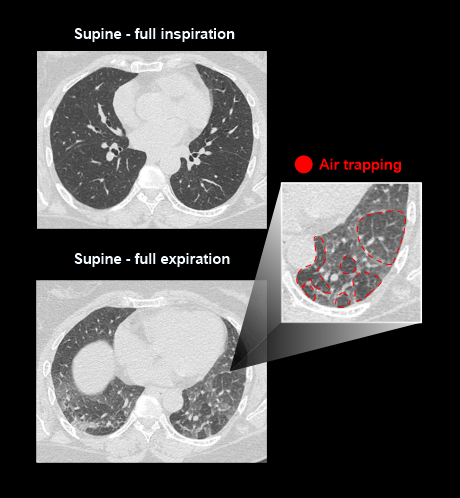
- Minimum intensity projection (MinIP) images with <10mm slab thickness, in transverse plane.
Explanation: helps to assess emphysema and air trapping.
Please review Chest non-contrast article for chest multiplanar reformation (MPR).
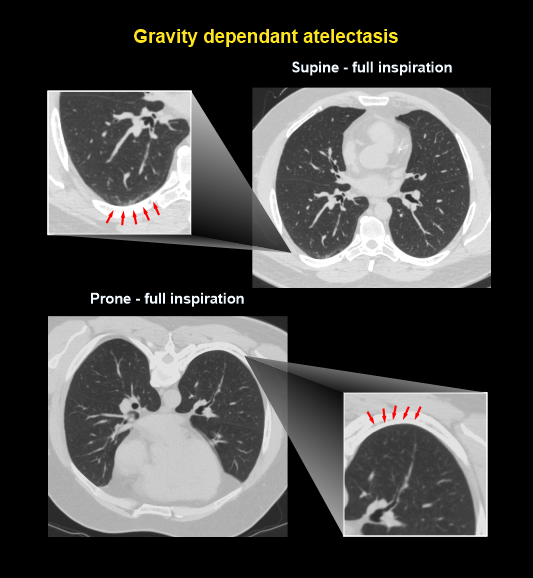
Additional scan steps such as supine, prone and full-expiration have their own benefits. In these steps, supine arrested expiration provides details to differentiate air trappings, and prone arrested inspiration can be used to separate posterior lung disease from atelectasis.
Reference
- Jane P. Ko, MD, Chair, Jonathan H. Chung, MD, & Paul Cronin, MB, BCh, BAO, FACR. (2020). ACR–SPR–STR Practice parameter for the performance of high-resolution computed tomography (HRCT) of the lungs.Retrieved from www.gravitas.acr.org.
- Chen A, Karwoski RA, Gierada DS, Bartholmai BJ, Koo CW. Quantitative CT Analysis of Diffuse Lung Disease. Radiographics.2020 Jan-Feb;40(1):28-43. doi: 10.1148/rg.2020190099. Epub 2019 Nov 29. PMID: 31782933.
- Sundaram B, Gross BH, Martinez FJ, Oh E, Müller NL, Schipper M, Kazerooni EA. Accuracy of high-resolution CT in the diagnosis of diffuse lung disease: effect of predominance and distribution of findings.AJR Am J Roentgenol. 2008 Oct;191(4):1032-9. doi: 10.2214/AJR.07.3177. PMID: 18806139.
- Hansell DM. Small airways diseases: detection and insights with computed tomography. Eur Respir J. 2001 Jun;17(6):1294-313. doi: 10.1183/09031936.01.00206101. PMID: 11491178.
- Nishino, M., Itoh, H., & Hatabu, H. (2014). A practical approach to high-resolution CT of diffuse lung disease.European journal of radiology, 83(1), 6–19. https://doi.org/10.1016/j.ejrad.2012.12.028
- Romanyukha, A., Nzitunga, P. S., & Dolcet, A. (2022, April 28). CT patient positioning plays key role in radiation dose reduction.www.auntminnie.com.
- Emilsson ÖI, Dessle A, Johansson H, Adeli S, Malinovschi A, Eloranta ML, Hansen T. Different chest HRCT scan protocols change the extent of ground glass opacities. BMC Pulm Med. 2022 Nov 21;22(1):430. doi: 10.1186/s12890-022-02212-7. PMID: 36404311; PMCID: PMC9677886.
- Burgel PR, Bergeron A, de Blic J, Bonniaud P, Bourdin A, Chanez P, Chinet T, Dalphin JC, DevillierP, Deschildre A, Didier A, Kambouchner M, Knoop C, Laurent F, Nunes H, Perez T, Roche N, Tillie-Leblond I, Dusser D. Small airways diseases, excluding asthma and COPD: an overview.Eur Respir Rev. 2013 Jun 1;22(128):131-47. doi: 10.1183/09059180.00001313. PMID: 23728867; PMCID: PMC9487373.
- Kazerooni EA. High-resolution CT of the lungs. AJR Am J Roentgenol.2001 Sep;177(3):501-19. doi: 10.2214/ajr.177.3.1770501. PMID: 11517038.