CT thoracic aortogram
Last updated May 13, 2026
Similar expressions
CT thoracic aortogram/ CT thoracic aorta angiogram/ CT thoracic angio/ CT aortogram/ CT thoracic aorta/ CT chest angiogram
Introduction
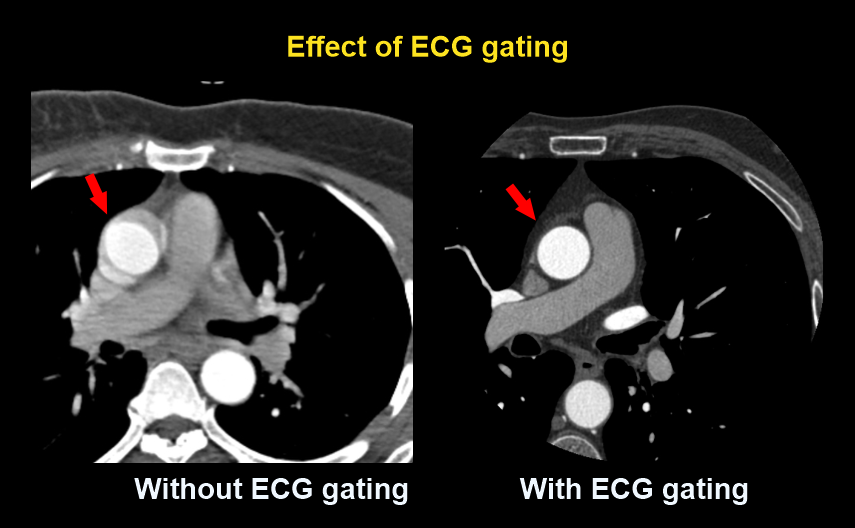
This study is performed to assess pathologies related with the thoracic aorta such as aortic aneurysms, stenosis, rupture, dissection and intra mural hematoma. Scan captures thoracic aorta from aortic arch up to diaphragm, but may be extended to common-iliac bifurcation, depending on patient’s condition. There are multiple phases in thoracic aortogram that perform before and after contrast injection. This scan differs from the abdominal angiogram because ECG triggering is used to avoid motion artifacts due to beating heart. Additionally, this scan can be used to assess coronary arteries, but only if the ECG gating is used.
Patient preparation
- Explain the procedure clearly and kindly.
- Remove metals related to the scanning area (underwear, necklaces).
- Practice breathing technique – breath in and hold during the scan.
Explanation: to avoid motion artifacts due to breathing.
- Check contraindications for contrast media administration and radiation exposure.
- Place an Intra venous (IV) cannula in a stable vein for contrast injection – green-18G cannula.
Explanation: Able to inject contrast at a higher rate through a green cannula.
- Place ECG electrodes avoiding interested region.
Explanation: ECG leads has metallic components that provide metallic artifacts. However, ECG gating helps to avoid aortic root motion artifacts.
Patient positioning
- Position the patient in supine and feet first on the imaging couch.
- Raise both hands above the head and place a positioning aid under them.
Explanation: hands beside the trunk give streak artifacts and increase radiation exposure.
- Keep the arm with the IV cannula strait.
Explanation: to facilitate contrast flow.
- Center the scanning area in the scanner iso-center [6].
Explanation: this reduces overall radiation exposure and increases image quality.
- Plan the scan starting point at the lower neck.
Scan planning
There are two steps in the scan, which are pre-contrast and arterial. Non-contrast phase is equallyimportant as contrast phase because it is used to identify conditions in aorta, including stents, calcifications and intramural hematoma (IMH). Although full coverage of thoracic aorta may not be needed in pre-contrast phase.
Chest arterial phase, which is nearly 25 seconds from contrast injection, changes according to the ejection fraction of the patient. Though either triggering or test bolus methods can be used to accurately initiate arterial phase. The former technique is explained in the end of this section while the latter is included in our pulmonary angiography article.
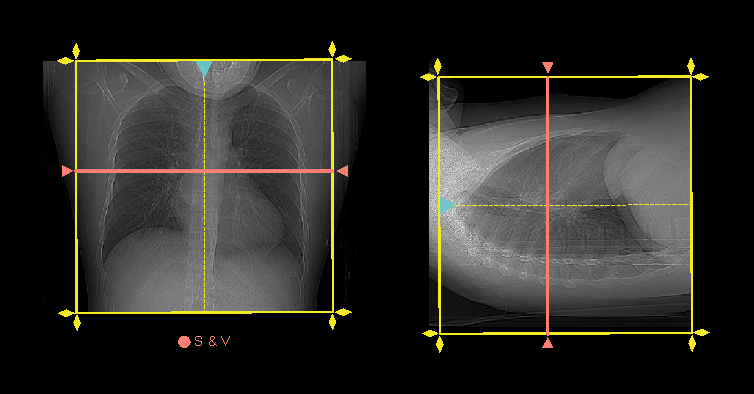
- Plan both scan slabs to cover from lung apex to posterior costophrenic sulci.
- Both phases are acquired under suspended full inspiration.
- Scan and view (S & V) slice is placed in the mid chest.
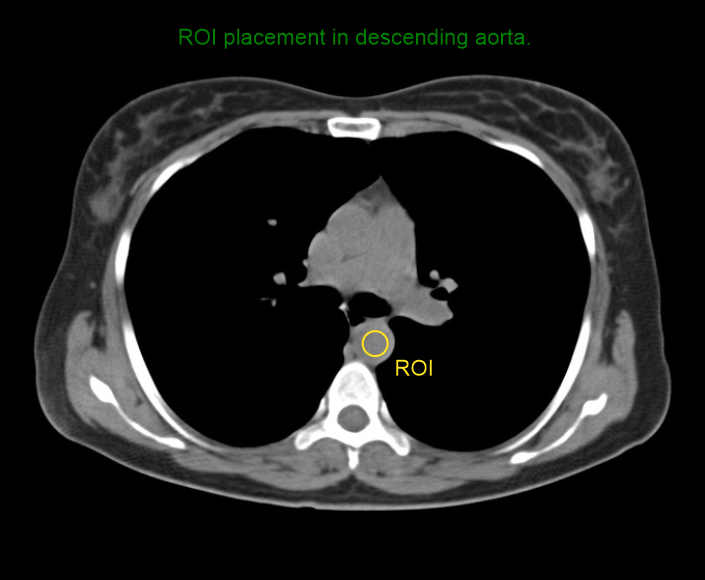
- Triggering region of interest (ROI) is placed in the descending aorta.
- Program the threshold value to 180 HU.
- Set S & V initiation delay to 10 seconds.
- Place no delay time for arterial scan.
Intravenous (IV) contrast infusion
- Inject 65-70 mL (65kg body weight, 640 slice scanner) of iodinated contrast at a rate of 4 – 4.5 mL/s.
- Inject 50-60 mL of saline flush following contrast injection - same injection rate.
Explanation: helps to flush out remaining contrast in veins and maintains the contrast flowfor a longer time.
Bolus tracking
In this method, ROI monitors live HU (Hounsfield units) value of descending aorta. As shown in the diagram, scan automatically starts when the monitoring HU value reaches the pre-planned threshold HU value.
ECG gating
Both prospective and retrospective triggering can be used for this scan, but they have their ownpros and cons. The former has lower radiation dose, but comparatively cardiac phase coverage is lesser than the latter. The latter has higher cardiac phase coverage, but radiation exposure is relatively higher than the former. Admittedly, prospective triggering offers diagnostically appropriate images from lower radiation exposure [2]. However, retrospective triggering may be used for functional analysis because it captures the whole cardiac cycle-reach our coronary angiography article for more information.
Post-processing
- Multiplanar reconstruction (MPR) images for all phases in soft-tissue window (WW: 400,WL:40), with slice thickness <5mm.
- Axial images in both lung (WW: 1500, WL: -500) and bone window (WW: 3500, WL: 350), with <3mm slice thickness.
Please refer to our chest non-contrast article for more images.
- Curved planar reformation (CPR) images of aorta.

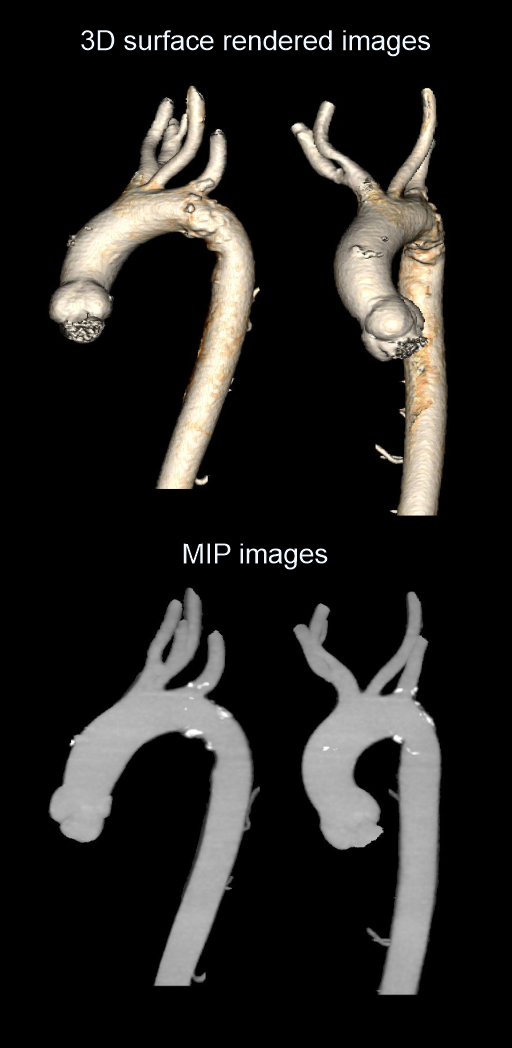
- Surface shaded images of aorta.
- Maximum intensity projection (MIP) images of aorta.
Reference
- Steven S. Raman, MD, Chair, Dorothy Gilbertson, MD, & Charles White, MD. (2021). ACR–NASCI–SIR–SPR Practice parameter for the performance and interpretation of body computed tomography angiography (CTA).Retrieved from www.gravitas.acr.org.
- Wu W, Budovec J, Foley WD. Prospective and retrospective ECG gating for thoracic CT angiography: a comparative study.AJR Am J Roentgenol. 2009 Oct;193(4):955-63. doi: 10.2214/AJR.08.2158. PMID: 19770316.
- Gavant ML, Flick P, Menke P, Gold RE. CT aortography of thoracic aortic rupture.AJR Am J Roentgenol. 1996 Apr;166(4):955-61. doi: 10.2214/ajr.166.4.8610581. PMID: 8610581.
- Jeffrey RB Jr. CT angiography of the abdominal and thoracic aorta.Semin Ultrasound CT MR. 1998 Oct;19(5):405-12. doi: 10.1016/s0887-2171(98)90017-8. PMID: 9800250.
- Ko JP, Goldstein JM, Latson LA Jr, Azour L, Gozansky EK, Moore W, Patel S, Hutchinson B. Chest CT Angiography for Acute Aortic Pathologic Conditions: Pearls and Pitfalls. Radiographics. 2021 Mar-Apr;41(2):399-424. doi: 10.1148/rg.2021200055. PMID: 33646903.
- Romanyukha, A., Nzitunga, P. S., & Dolcet, A. (2022, April 28). CT patient positioning plays key role in radiation dose reduction.www.auntminnie.com.
- Shen, Y. H., LeMaire, S. A., Webb, N. R., Cassis, L. A., Daugherty, A., & Lu, H. S. (2020). Aortic Aneurysms and Dissections Series.Arteriosclerosis, thrombosis, and vascular biology, 40(3), e37–e46. https://doi.org/10.1161/ATVBAHA.120.313991
- Guglielmi, V., Rinkel, L. A., Groeneveld, N. S., Lobé, N. H., Boekholdt, S. M., Bouma, B. J., Beenen, L. F., Marquering, H. A., Majoie, C. B., Roos, Y. B., van Randen, A., Planken, R. N., & Coutinho, J.M. (2020). Mind the Heart: Electrocardiography-gated cardiac computed tomography-angiography in acute ischaemic stroke-rationale and study design.European stroke journal, 5(4), 441–448. https://doi.org/10.1177/2396987320962911