CT Neck with Contrast
Last updated June 27, 2026
By Radiohelp Staff
Similar expressions
CT neck contrast/ CECT neck/ CT contrast neck protocol
Introduction
CECT Neck is used for the assessment of congenital abnormalities, neoplasms and palpable masses. Usually, scan is performed with multiple phases, including non-contrast and post-contrast phases.
Patient preparation
- Explain the procedure kindly and clearly.
- Remove metal related to the neck area (necklaces, undergarments).
- Instruct the patient to be steady and not to swallow during the procedure.
- Ask to breath slowly during the procedure.
- Assess the ability to administer contrast media and expose radiation.
- Place a cannula in a stable vein for contrast injection – pink-20G cannula.
Patient positioning
- Position in head-first and supine.
- Extend the neck slightly.
Explanation: reduces streak artifacts or beam hardening artifacts due to the lower jaw. Same results can be achieved by angulating CT gantry.
- Position the shoulders in a pulled down position and arms next to the body.
Explanation: reduces streak artifacts or beam hardening artifacts due to wide shoulders. Placing a cushion under mid-upper thorax moves shoulders posteriorly, and helps to reduce streak artifacts at the root of the neck [2].
- Hand which is used to infuse contrast media is placed straight to facilitates contrast flow.
- Center the scanning area in the scanner iso-center [5].
Explanation: this reduces overall radiation exposure and increases image quality.
- Plan the scout starting point at the nipple level.
Scan planning
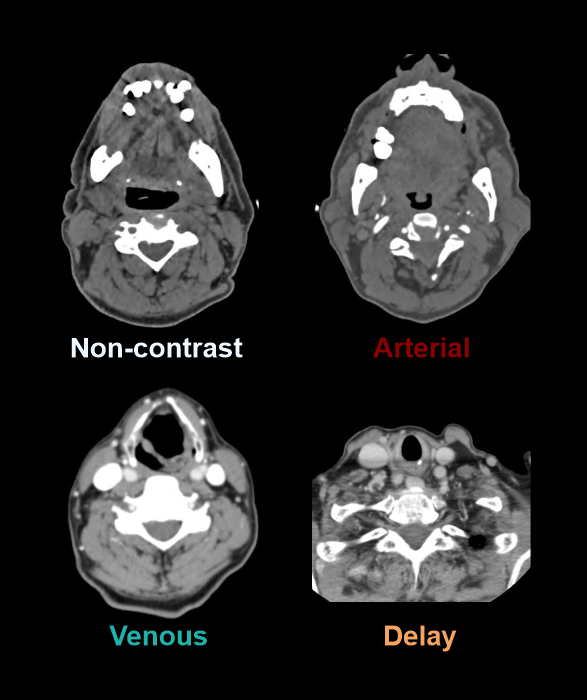
Three to four phases are performed: pre-contrast, arterial phase, venous phase and/or Delayed phase.
- For all phases, plan the scan slab to cover from the skull base to the top of the aortic-arch.
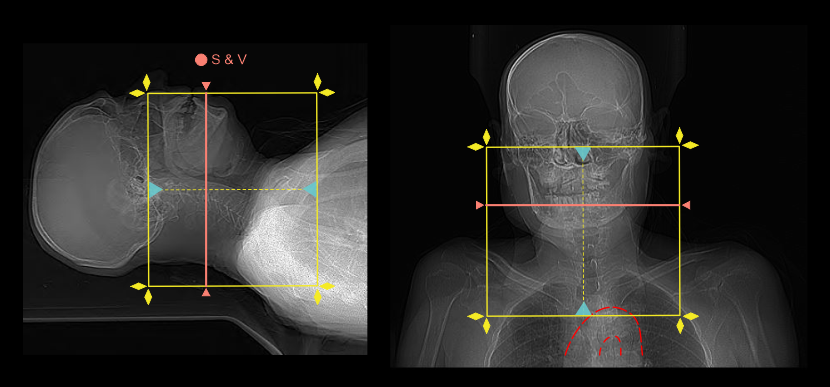
- For studies to assess vocal cord palsy, the inferior extent of the scan area should extend to aortopulmonary window or carina.
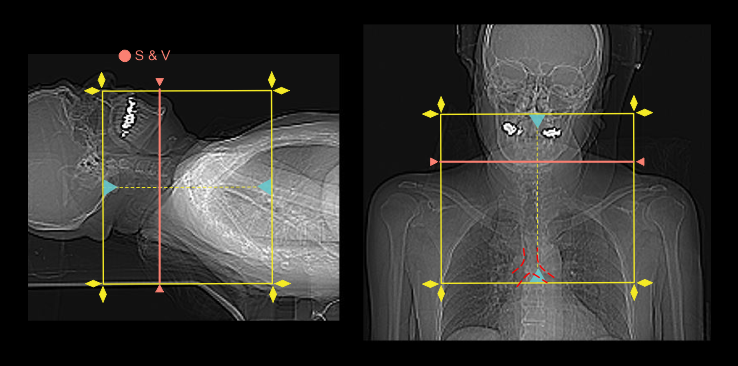
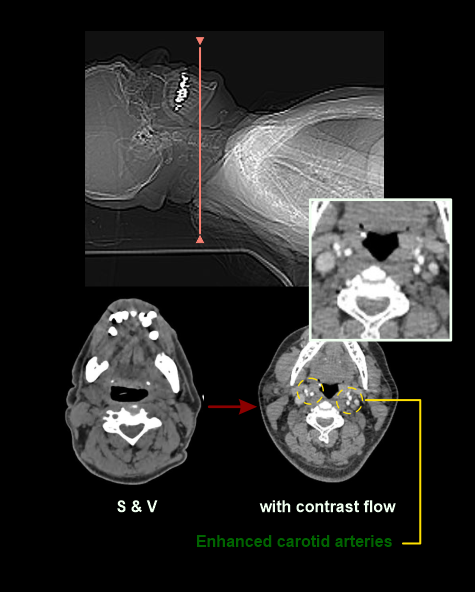
Triggering or bolus tracking method can be used to initiate the arterial phase because arterial enhancement can be viewed in real-time from the scan and view (S & V) slice, avoiding early or delay acquisitions. Manual start without ROI is recommended because it is challenging to recognize carotid arteries in pre-contrast S & V slice.
- Place the S & V slice at the mid part of the neck.
- Set S & V initiation time to 5 seconds from the contrast injection.
- Plan the scan direction for arterial phase from head to foot.
Explanation: this direction avoids delayed acquisition of superior neck area, visualizing veins and evades streak artifacts at the root of the neck when there is undiluted contrast media in brachiocephalic and subclavian veins.
- Plan the scan direction for venous phase from foot to head with a 2 second delay.
Explanation: this is to avoid further delay because venous phase starts at the point where the arterial phase ends, skipping the time it takes to move to the skull base.
- Place a 3-5 min delay time for the delayed phase.
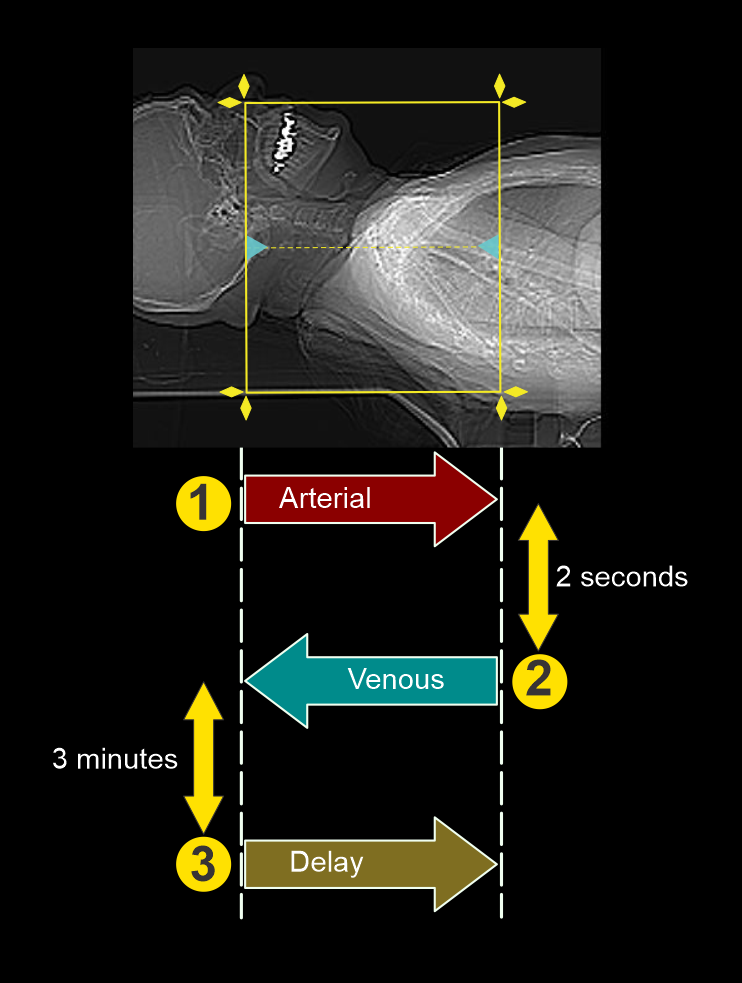
- Manually start the scan when you see adequate carotid enhancement.
Intravenous (IV) contrast infusion
- Pressure injector is used to inject 50-60 ml of iodinated contrast media at a flow rate of 3ml/s.
- Inject 40-50ml saline chase following contrast media infusion at the same infusion rate.
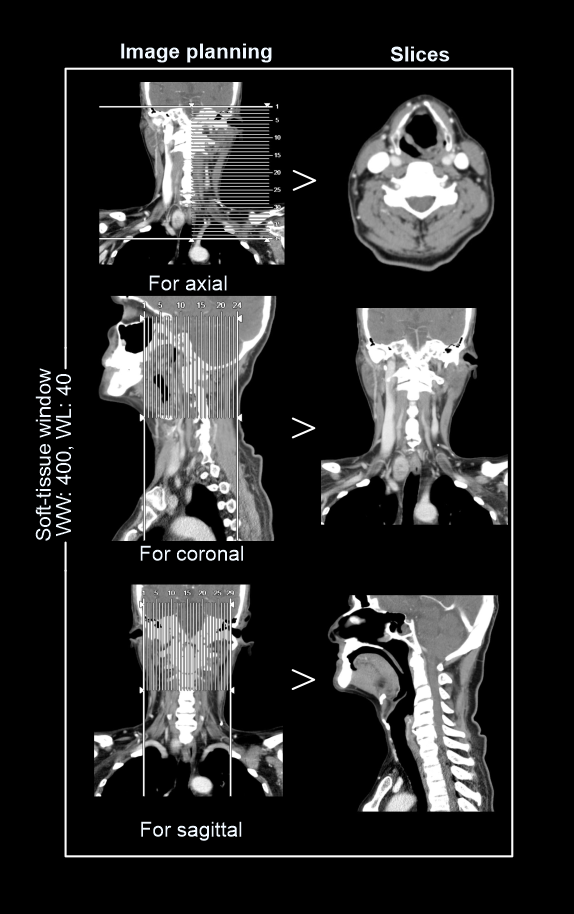
Post-processing
- Axial, coronal and sagittal images in soft-tissue window (WW: 400, WL:40), without exceeding 3mm slice thickness.
- Additionally, a suitable image in bone (WW: 3500, WL:350) window, displayed in any plane, without exceeding 3mm slice thickness.
- For vocal cord neoplasms, 1mm thin sections of multi planer reformats (MPR) are helpful insoft-tissue window limited to the larynx, and axial slices are reformatted parrel to the vocal cords or hyoid bone – refer Neck non-contrast article for images.
Reference
- Ashley H. Aiken, MD, Chair, Paul M. Bunch, MD, & Kavita K. Erickson, MD. (2021). ACR–ASNR–SPR Practice parameter for the performance of computed tomography (CT) of the extracranial head and neck.Retrieved from www.gravitas.acr.org.
- Harvey, G. D., Mayer, D. P., & Radecki, P. D. (1984). Simplified patient positioning to reduce beam hardening in CT of the lower neck. AJNR. American journal of neuroradiology, 5(6), 796.
- Groell, R., Willfurth, P., Schaffler, G. J., Mayer, R., Schmidt, F., Uggowitzer, M. M., Tillich, M., & Genser, B. (1999). Contrast-enhanced spiral CT of the head and neck: comparison of contrast material injection rates.AJNR. American journal of neuroradiology, 20(9), 1732–1736.
- Groell R, Doerfler O, Schaffler GJ, Habermann W. Contrast-enhanced helical CT of the head and neck: improved conspicuity of squamous cell carcinoma on delayed scans.AJR Am J Roentgenol. 2001 Jun;176(6):1571-5. doi: 10.2214/ajr.176.6.1761571. PMID: 11373235.
- Romanyukha, A., Nzitunga, P. S., & Dolcet, A. (2022, April 28). CT patient positioning plays key role in radiation dose reduction.www.auntminnie.com.